Autologous Reconstruction
Using your body's own tissue for microsurgical breast reconstruction, such as DIEP flap, PAP flap, TUG flap, and autologous fat grafting, among other advanced reconstructive techniques.

Restoring Natural Form Through Microsurgery
As a dual board-certified plastic surgeon based in Austin, Texas, my commitment is to offer patients the most advanced breast reconstruction options - including microsurgery. The profound physical and emotional impact of a cancer and mastectomy require a reconstructive approach that prioritizes long-term health, natural aesthetics, and structural integrity. Autologous breast reconstruction—often referred to as "flap" surgery—achieves these goals by repurposing the patient's own skin and fat, completely avoiding the use of prosthetic implants.
This methodology represents the gold standard in restorative plastic surgery. My background, encompassing rigorous surgical training at the University of Michigan and medical education at Baylor College of Medicine, drives a commitment to evidence-based, precision surgery. Furthermore, my active involvement in research and education ensures that my practice consistently integrates the latest advancements in surgical science and patient safety protocols.
What is the advantage of autologous or DIEP flap breast reconstruction?
The fundamental advantage of autologous reconstruction is longevity and natural integration. Unlike silicone or saline implants, which carry inherent risks of foreign body, capsular contracture, rupture, and the potential / eventual need for surgical replacement, living tissue grows, ages, and fluctuates in weight identically to the rest of the body. Once the transferred tissue successfully integrates and heals, the reconstructed breast provides a permanent, lifelong solution.
Furthermore, the use of living tissue restores a natural warmth, softness, and anatomical drape that synthetic materials cannot fully replicate. For patients requiring post-mastectomy radiation therapy (PMRT), autologous tissue withstands radiation significantly better than implants and may restore more natural tissue behavior in the radiated tissues. The robust blood supply of a living tissue flap drastically reduces the severe complication rates—such as deformity, skin necrosis or severe contracture—often associated with irradiated prosthetic reconstructions.
Advanced Perforator Flap Techniques
Modern autologous reconstruction relies heavily on nerve and muscle-sparing perforator flap techniques. These highly specialized procedures meticulously isolate the necessary skin and fat along with their specific, microscopic blood vessels (perforators), completely sparing the underlying muscle structure at the donor site. This modern approach minimizes donor site morbidity, accelerates recovery times, and preserves the patient's core physical strength.
What is a DIEP flap?
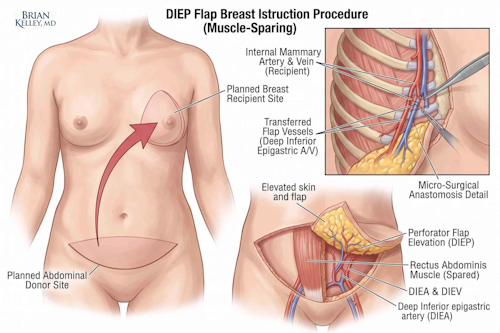
The Deep Inferior Epigastric Perforator (DIEP) flap is the most commonly performed and highly regarded method of autologous reconstruction. This procedure utilizes the excess skin and adipose tissue from the lower abdomen. The tissue block, along with the deep inferior epigastric artery and vein, is completely detached and transplanted to the chest. Utilizing a high-powered operating microscope, these tiny vessels are meticulously reconnected to the internal mammary vessels located in the chest wall. Because the rectus abdominis (the central abdominal muscle) is left largely intact, patients retain full core functionality while benefiting from a secondary contouring effect at the donor site, aesthetically similar to a cosmetic abdominoplasty. The trade off is scars and surgical risks to the donor site - in this case, scars on your lower tummy and around the belly button.
What is a PAP flap?
For patients who lack sufficient abdominal tissue, or those who have undergone prior abdominal surgeries that preclude the use of a DIEP flap, the Profunda Artery Perforator (PAP) flap serves as an excellent, muscle-sparing alternative. The PAP flap harvests required tissue from the upper posterior thigh, just below the gluteal fold. This technique leaves a discreet, easily hidden scar within the natural crease of the lower buttock and upper thigh, providing ample volume to construct a natural-appearing breast mound without sacrificing any critical leg muscle or impacting mobility.
What is a TUG flap?
The Transverse Upper Gracilis (TUG) flap is an additional secondary option utilizing tissue from the inner thigh. This flaps main drawbacks, compared to other autologous reconstruction options, are that a donor muscle is often required and the volume is often lower. While the traditional gracilis flap sometimes necessitates incorporating a small segment of the gracilis muscle, advanced variations aim to spare as much functional muscle as clinically possible. The TUG flap is particularly well-suited for patients seeking small to moderate breast volumes. It offers the secondary benefit of an inner thigh lift contouring effect, though it requires precise patient selection to ensure adequate tissue availability.
What is "fat grafting" and why might I need it?
Autologous fat grafting is an indispensable adjunct procedure utilized extensively in both implant-based and autologous reconstructions. This specialized technique involves harvesting fat via low-pressure liposuction from donor areas such as the flanks, thighs, or abdomen. The harvested fat cells are then purified and strategically injected in small, precise aliquots into the reconstructed breast. Fat grafting is essential for refining topographical contours, filling minor depressions or step-offs, correcting mild asymmetry, and optimizing the final aesthetic result to perfectly mimic the natural slope and projection of the native breast. It is particularly effective and important in patients with a history of radiation treatment.
The Surgical Journey - what is the timeline for autologous breast reconstruction?
The decision to undergo microsurgical breast reconstruction requires thorough, highly individualized preoperative planning. The initial consultation involves a meticulous review of the patient's oncologic history, anatomical suitability, and personal reconstructive goals. Advanced vascular imaging, such as CT angiography (CTA), is routinely utilized to map the precise anatomical location and caliber of the perforator blood vessels prior to making any incisions. This technological integration ensures the safest and most efficient surgical execution possible.
The operative procedure itself is highly complex, often lasting between four to eight hours depending on whether the reconstruction is unilateral (one breast) or bilateral (both breasts). Other factors like perforator anatomy, obesity, radiation, or other scarring / technical challenges can increase the time needed for surgery. Postoperative care requires a hospital stay of usually a few days in a specialized unit, where nursing staff trained in microsurgery continually monitor the blood flow to the newly transferred tissue using specialized Doppler equipment or light spectroscopy. Total recovery, enabling a full return to all baseline physical activities and rigorous exercise, generally spans six to eight weeks in most patients and may require physical therapy consultation.
What are likely outcomes of autologous or DIEP flap breast reconstruction?
Achieving excellence in microsurgical breast reconstruction requires technical mastery, extensive operative experience, and an unwavering commitment to patient safety and long-term oncologic health. The intersection of an active clinical practice in Austin and ongoing academic research facilitates a surgical environment where safety protocols, aesthetic outcomes, and patient education are continuously optimized.
Providing a definitive, lifelong reconstructive solution allows patients to decisively close the chapter on their active surgical cancer treatment. The utilization of autologous tissue not only restores physical form but plays a critical role in psychological restoration, offering a durable, natural result that lasts a lifetime.
Written by Brian P. Kelley, MD — Dual Board-Certified Plastic & Hand Surgeon
Medically reviewed: May 4, 2026 · Last updated: May 4, 2026
Educational content. Not a substitute for individualized medical evaluation.
Related Topics
- Blog Post on DIEP flap breast reconstruction
- Differences Between TRAM and DIEP Flap Reconstruction
- Recovery Guide for DIEP Flap Reconstruction
- Implants and Implant-based Reconstruction
- Blog Post on Implant-based breast reconstruction
- Oncoplastic breast reconstruction
- Post-Mastectomy Breast Sensation
- Autologous Fat Grafting
- Facial and Mohs reconstruction
- Extremity reconstruction and limb salvage
- Lymphovenous Bypass for Post-Mastectomy Lymphedema
Closing Disclaimer
This article is educational and does not establish a doctor-patient relationship. It does not replace individualized consultation, examination, or review of personal medical history. Patients with sensory changes or pain after mastectomy are encouraged to discuss their specific situation with their oncology team and, when appropriate, with a plastic surgeon experienced in nerve and breast surgery.
DIEP and Autologous reconstruction
FAQs
Frequently Asked Questions About Autologous Reconstruction
DIEP flap reconstruction uses the patient's own abdominal tissue, while implant reconstruction uses a saline or silicone device. DIEP avoids a foreign implant, reshapes the abdomen as a secondary effect, and tolerates radiation better. Implants involve a shorter operation and no donor site, but carry their own long-term considerations including capsular contracture and revision.
DIEP flap reconstruction following mastectomy for breast cancer is generally covered under the federal Women's Health and Cancer Rights Act of 1998, which requires group health plans that cover mastectomy to also cover reconstruction. Coverage details, in-network status, and prior authorization requirements vary by plan and should be confirmed with the insurer before scheduling.
Sensation after DIEP flap reconstruction is variable and incompletely characterized in the literature, even after dedicated nerve restoration procedures. Some patients regain meaningful protective and tactile sensation over a year or more; others have persistent numbness. The literature lacks consistent data delineating normative values for breast sensibility, which limits what any surgeon can promise.
DIEP flap surgery duration depends on whether the reconstruction is unilateral or bilateral and whether it is performed immediately with mastectomy or delayed. Most cases are long operations measured in hours rather than minutes, followed by inpatient admission for flap monitoring. The operating surgeon can give a more precise range based on the specific plan.
Practices vary, and the literature is not uniform. Some centers have implemented protocols to temporarily stop tamoxifen before microvascular breast reconstruction based on concerns about thromboembolic risk and flap complications. The decision should be made jointly by the plastic surgeon and the medical oncologist for each individual patient. You may be asked to hold other medications, especially for anesthesia and bleeding safety.
Out-of-state or out-of-city patients undergoing DIEP flap reconstruction in Austin typically remain locally for at least two to three weeks after surgery, encompassing the inpatient stay, drain management, and the initial postoperative visits. The exact duration is determined by the surgeon based on healing and travel safety, particularly the risk of venous thromboembolism on long flights. If you live nearby, we can manage this recovery with short trips into town, but you will need help with transporation.
Return to work after DIEP flap surgery typically depends on the physical demands of the job. Patients in desk-based roles often return part-time around the three to six week mark, while those in physically demanding occupations require longer. Lifting restrictions and core healing dictate the timeline, not pain alone. In select rare cases, we may coordinate lifting of restrictions with your progression with physical therapy.
A prior C-section likely does not disqualify a patient from DIEP flap surgery. The cesarean scar can affect the abdominal skin envelope and occasionally the perforator vessels, but most patients with prior cesarean delivery remain candidates. Preoperative CT angiography is used to map the perforators and confirm that the anatomy supports a safe reconstruction.
A prior tummy tuck often does disqualify a patient from DIEP flap surgery. The tummy tuck is specifically designed to remove the tissue we need to rebuild the breast. Preoperative CT angiography is used to map the blood vessels and confirm if the anatomy supports a safe reconstruction. If not, alternative autologous flaps (TUG, PAP, ALT, SGAP, latissimus dorsi, etc) can be used or we can often safely proceed with implant-based reconstruction if needed.
Want to learn more?
Book a consultation
