Facial and Mohs Reconstruction in Austin, TX
Facial reconstruction after cancer treatment focuses on restoring both function and aesthetic appearance. This involves intricate procedures to rebuild vital facial structures, ensuring patients regain confidence and quality of life.

Introduction
Facial skin cancers are common in central Texas. The combination of intense year-round sun exposure, an aging population, and high outdoor activity produces a steady stream of basal cell carcinomas, squamous cell carcinomas, melanomas, and the rarer Merkel cell carcinomas — many of which present on the face, scalp, ears, and neck where the cosmetic and functional consequences of surgical removal are highest. Reconstruction is the second half of that treatment.
I practice as a dual board-certified plastic and hand surgeon in Austin, Texas, with academic Affiliate Faculty appointments at Dell Medical School and as a partner with the Seton Institute for Reconstructive Plastic and Hand Surgery. Mohs reconstruction, head and neck oncologic microsurgery, and reconstruction following melanoma and other oncologic resection are explicit clinical focuses of my practice. My published work in this area includes a peer-reviewed paper on nasal lining reconstruction using a superior labial artery mucosal flap — a technique relevant to full-thickness nasal defects after Mohs — and a review on the evaluation and reduction of nasal trauma.
This page covers the major regions of the face that require reconstruction after skin cancer excision, the principles that guide the choice of reconstruction, and the coordination with the dermatologic or surgical oncology team that typically removes the cancer. For broader skin cancer biology and screening, those topics are managed primarily by dermatology and not covered here.
How the Patient Pathway Usually Works
Most patients who arrive for facial reconstruction have already undergone — or are scheduled to undergo — biopsy and Mohs micrographic surgery by a fellowship-trained Mohs surgeon, or wide local excision by a surgical oncologist. The cancer team focuses on clearing the cancer with negative margins. The reconstructive surgeon focuses on closing the resulting defect with the best functional and cosmetic outcome the situation allows.
The two specialties usually coordinate by either of two pathways. In the first, the patient sees the Mohs surgeon in the morning, has the cancer excised with margins confirmed clear, and is then sent or referred for reconstruction the same day or within a day or two. In the second, surgical oncology performs wide local excision and reconstruction in a single combined operation, sometimes with sentinel lymph node biopsy in the same setting. The right pathway depends on the cancer type, location, expected defect size, and patient preference.
For melanoma in particular, sentinel lymph node biopsy is often performed as part of the oncologic workup. Depending on the timing and the team, this may be combined with the reconstruction or staged separately. The decision is made between the surgical oncologist and the patient, with input from medical oncology when systemic disease assessment is relevant.
Region-by-Region Reconstruction
The face is not one tissue; it is a mosaic of regions with distinct anatomy, distinct functional demands, and distinct reconstructive options. The discussion below covers the most common areas.
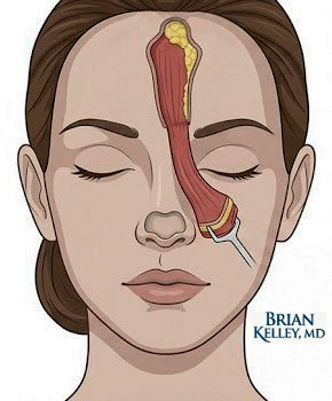
Nose
The nose is the most reconstructively demanding region of the face and the most common site for Mohs surgery. Defects can involve skin alone, skin and cartilage, or full-thickness loss including nasal lining. Small superficial defects often close primarily or with a local flap (bilobed, dorsal nasal, nasolabial). Larger defects require regional flaps — the paramedian forehead flap remains the workhorse for substantial nasal reconstruction. Full-thickness defects need three-layer reconstruction: external skin cover, structural cartilage support, and an internal lining. My peer-reviewed work on the superior labial artery mucosal flap, published in the Journal of Craniofacial Surgery, described an alternative source of nasal lining that can be used in selected reconstructions.
Eyelid and Periocular Region
Eyelid reconstruction has functional implications that other facial regions do not — the eyelids must close completely to protect the cornea, and the lid margin must align precisely. Reconstruction options range from primary closure for very small defects to advancement and rotation flaps from adjacent skin, full-thickness skin grafts from the contralateral eyelid or supraclavicular area, and tarsoconjunctival flaps for posterior lamellar reconstruction. Coordination with oculoplastic surgery is often appropriate when the tear duct system is involved.
Ear
Ear reconstruction balances the cartilaginous architecture against thin overlying skin. Small defects can be reconstructed with wedge resection and primary closure, antihelical or helical advancement flaps, or skin grafts. Larger defects involving cartilage may require multi-stage reconstruction with cartilage grafts from the contralateral ear or rib, or with regional flaps from the postauricular skin. The aesthetic goal is symmetry with the contralateral ear, which is the visible reference.
Scalp and Forehead
The scalp has unique reconstructive challenges. The skin is thick and inelastic, the underlying galea limits stretch, and the calvarium beneath is unforgiving when wound coverage fails. Small defects close primarily; moderate defects require local rotation or transposition flaps; large defects sometimes require tissue expansion or, in the most severe cases, free tissue transfer to provide enough vascularized coverage. Forehead defects are reconstructed with similar principles but with closer attention to symmetry of the brow line and the hairline.
Mouth and Lip
Lip reconstruction must restore the vermilion border, the oral competence that prevents drooling, and the appearance of a symmetric mouth. Small defects can be closed primarily or with vermilion advancement. Defects involving up to a third of the lip can often be reconstructed with full-thickness wedge excision and primary repair. Larger defects require named lip flaps — Abbe, Estlander, Karapandzic, or stair-step rotational flaps — with the choice depending on the location and extent of the defect.
Neck
Cervical reconstruction following neck dissection or skin cancer excision in the neck region uses regional skin advancement, cervicofacial rotation flaps, and occasionally regional pedicled flaps from the chest or back. The anatomy here demands particular attention to the great vessels and the marginal mandibular branch of the facial nerve.
Skin Cancer of the Hand
Skin cancers occur on the dorsal hand, fingers, and nail beds in addition to the face. These lesions are sometimes excised by Mohs surgery, sometimes by surgical oncology, and the reconstructive demands are distinct. Hand defects after skin cancer excision can require skin grafts, local flaps, regional flaps, or in larger defects, free tissue transfer. The combination of dual training in plastic and hand surgery is particularly useful here — the reconstructive surgeon needs both the soft-tissue expertise of plastic surgery and the functional anatomy expertise of hand surgery to close a hand defect without compromising tendon glide, joint motion, or sensation.
Coordination with Sentinel Lymph Node Biopsy
For melanoma, Merkel cell carcinoma, and selected squamous cell carcinomas, sentinel lymph node biopsy is part of staging. The biopsy is performed by surgical oncology, typically in the same operative setting as the wide local excision when timing allows. The reconstruction is then planned around the timing of the biopsy result — many patients can have definitive reconstruction at the same setting, while others may have a staged approach if the lymph node result will alter the systemic treatment plan or if larger margins may be needed.
Outcomes
Facial reconstruction outcomes are evaluated on three dimensions: oncologic safety, function, and appearance. Oncologic safety is established before reconstruction begins — the cancer team confirms negative margins, and the reconstructive surgeon does not begin closure on tissue that has not been cleared. Function is preserved by matching the reconstruction to the demands of the affected region — a lid that closes, a nose that breathes, a lip that seals. Appearance is the dimension on which patients judge results most directly.
The honest framing is that facial reconstruction is restoration, not replacement. Even an excellent reconstruction does not return the face to its pre-cancer appearance, particularly after substantial defects. Scars, contour changes, and visible color or texture differences are common and usually accepted as the trade-off for cancer clearance. Smaller defects in less visible regions often heal to results that are difficult to detect at conversational distance. Larger reconstructions, particularly nasal and ear reconstructions, may benefit from secondary refinement procedures months later.
Risks
The risks of facial reconstruction overlap with general surgical risks: bleeding, hematoma, infection, wound dehiscence, and unsatisfactory scar formation. Region-specific risks include partial flap loss (more likely in smokers, in patients with prior radiation, or when flap circulation is marginal), distortion of nearby features (lid retraction after periocular reconstruction, nasal valve narrowing after nasal reconstruction, lip incompetence after lip reconstruction), and persistent contour irregularity. Recurrence of skin cancer is determined by the original oncologic resection rather than the reconstruction, but reconstruction can occasionally complicate later cancer surveillance by altering the appearance of the surgical bed.
Written by Brian P. Kelley, MD — Dual Board-Certified Plastic & Hand SurgeonMedically reviewed: May 4, 2026 · Last updated: May 4, 2026Educational content. Not a substitute for individualized medical evaluation.
Frequently Asked Questions
Will I have a visible scar after Mohs reconstruction?
Yes. Every reconstructive surgery produces a scar. The goal is to place the scar along natural relaxed skin tension lines and at the borders between aesthetic units of the face, where it is least visible. Scar appearance continues to improve for a year or more after surgery. Most patients find the final scar acceptable, particularly compared to the alternative of an open wound or untreated cancer.
How soon after Mohs surgery should reconstruction be performed?
For most defects, reconstruction is performed the same day or within a day or two of Mohs surgery. Some larger or complex defects benefit from a brief delay to allow swelling to subside or to plan a multi-stage reconstruction. The Mohs surgeon and reconstructive surgeon coordinate the timing.
What is the difference between Mohs surgery and wide local excision?
Mohs micrographic surgery removes the cancer in stages with same-day microscopic examination of all margins, allowing precise tissue conservation while ensuring clear margins. Wide local excision removes the cancer with a predetermined margin and sends the specimen for standard pathology, which produces the result over days. Mohs is preferred for facial cancers and for tumors with poorly defined borders. Wide excision is standard for melanoma and for cancers where Mohs is not appropriate.
Will I need additional surgery to refine the reconstruction?
Many patients do not. Some larger reconstructions — particularly multi-stage nasal reconstruction — are planned with anticipated revision procedures. Smaller reconstructions occasionally benefit from minor revision for scar refinement, contour adjustment, or symmetry. The decision to revise is made together with the patient several months after the initial reconstruction. If we are worried about the cancer being completely excised, we might delay definitive reconstruction or stage the procedure.
Can skin cancers on the hand be reconstructed the same way as facial cancers?
The same general reconstructive principles apply, but the priorities differ. Hand reconstruction prioritizes preservation of tendon glide, joint motion, and sensation in addition to cosmetic considerations. Plastic and hand surgery training together provides the right combination of expertise for this work.
Medical References
- Momoh AO, Kelley BP, Diaz-Garcia R, et al. An Alternative Mucosal Flap for Nasal Lining: The Superior Labial Artery Mucosal Flap — An Anatomic Study. Journal of Craniofacial Surgery. 2013;24(2):626–628. PMID: 23524761.
- Kelley BP, Downey CR, Stal S. Evaluation and Reduction of Nasal Trauma. Seminars in Plastic Surgery. 2010;24(4):339–347. PMID: 22550458.
- Cho KY, Kelley BP, Monier D, et al. TRPS1 Regulates Development of Craniofacial Skeleton and Is Required for the Initiation of Palatal Shelves Fusion. Frontiers in Physiology. 2019;10:513. PMID: 31130868.
- American Society of Plastic Surgeons — skin cancer reconstruction resources: https://www.plasticsurgery.org/.
- American College of Mohs Surgery — patient resources: https://www.mohscollege.org/.
Related Topics
- Core and pelvic reconstruction
- Extremity reconstruction and limb salvage
- Hand and wrist surgery overview
- General Facial and Body Reconstruction
- Autologous Fat Grafting
- Post-operative Pain Treatment and Nerves
Closing Disclaimer
This article is educational and does not establish a doctor-patient relationship. It does not replace individualized consultation, examination, or review of personal medical history. Patients with facial skin cancers, Mohs defects, or post-oncologic facial reconstruction needs are encouraged to schedule a consultation to discuss their specific situation and reconstructive options.
Patient Testimonials
What are patient's saying about Dr Kelley?
Excelente cirujano! Muchas gracias! Bendiciones al equipo.
Maria Acevedo Espinoza
Want to learn more?
Book a consultation
