Peripheral Nerve Surgery and Reconstruction
In the endeavor to restore both form and function, we offer the state-of-the-art in precision nerve reconstruction enables the restoration of movement, alleviation of pain, and a return to cherished activities.

Services Offered
Techniques including nerve repair, decompression, reconstruction, pain management, enhanced recovery, functional replacement, or facilitation of myoelectric prostheses
Nerve Repair and Reconstruction
Microsurgical nerve reconstruction and repair using state-of-the-art techniques
Nerve and Tendon Transfer
Restoring function and use with customized synergistic transfers
Pain Alleviation and Advanced Prostheses for Amputees
Treatment of neuromas and options for myoelectric prostheses - TMR and RPNI
Nerve Decompression
Treatment of nerve entrapment or compression syndromes
From the Blog

21.6.2026
Nerve Pain After Knee or Hip Replacement: The Overlooked Diagnosis
Persistent pain after knee or hip replacement isn't always the implant. Dr. Brian Kelley, an Austin nerve surgeon, explains the overlooked nerve diagnosis — infrapatellar saphenous neuroma after knee replacement, meralgia paresthetica after hip replacement, and peroneal nerve injury causing foot drop. Covers how to tell nerve pain from mechanical joint problems, why ruling out the joint comes first, who benefits from surgery, and an honest look at the evidence.

5.6.2026
Nerve Pain After Breast Cancer Radiation and Mastectomy: When Surgery Helps
Struggling with chronic chest or arm pain after breast cancer? Austin-based peripheral nerve specialist and breast reconstruction surgeon Dr. Brian P. Kelley explains how post-mastectomy neuromas and radiation neuritis—not your breast reconstruction — may be the true cause. We discuss evidence-based treatments and options for advanced nerve surgeries like TMR and RPNI. Learn how targeted nerve surgery might provide meaningful pain relief while potentially preserving your breast reconstruction.

2.6.2026
Nerve Transfers vs. Nerve Grafts: How Surgeons Choose
Nerve graft or nerve transfer? Dr. Brian Kelley, dual board certified nerve surgeon in Austin, walks through the two strategies, where each works best, and how the choice is actually made — covering motor and sensory nerves, hand and brachial plexus and lower-extremity considerations, modern adjuncts including processed nerve allograft, and why timing matters. Patient-reported outcomes data and a framework for selecting a surgeon included.
Peripheral Nerve Surgery, RPNI, and TMR
Written by Brian P. Kelley, MD — Dual Board-Certified Plastic & Hand Surgeon
Medically reviewed: May 3, 2026 · Last updated: May 3, 2026
Educational content. Not a substitute for individualized medical evaluation.
Introduction
Peripheral nerve injuries change lives in ways that other injuries cannot match. A single transected digital nerve can mean the loss of a fingertip's sensation. A brachial plexus injury after a motorcycle crash can mean an arm that hangs limp. An amputation can mean years of phantom pain and the inability to use a prosthetic comfortably. As a dual board-certified plastic and hand surgeon in Austin, Texas, I hold Affiliate Faculty positions at Dell Medical School at The University of Texas at Austin and serve as an attending surgeon at the Seton Institute of Reconstructive Plastic and Hand Surgery. Peripheral nerve surgery is a significant aspect of my practice - addressing issues from congenital injuries, cancer, or trauma.
This page explains how nerve repair and reconstruction work, why timing matters, what Regenerative Peripheral Nerve Interface (RPNI) and Targeted Muscle Reinnervation (TMR) offer to amputation patients, and how the approach differs between children and adults. I treat both populations, and the biological differences between them shape the surgical strategy substantially.
Why Nerve Healing Is Different
Most cells in the human body are biologically isolate - what you're looking at is the cell. A skin cell, a muscle cell, a liver cell — each carries its own nucleus and can divide locally to repair injury right where you see them. Peripheral nerves do not work this way, and that fact governs everything about how we treat them.
A motor nerve cell's nucleus — its control center — sits in the anterior horn of the spinal cord. The axon is the long cable extending from that nucleus to the muscle it controls. In an adult, that microscopically narrow cable can be more than a meter long - creating an incredibly delicate and fragile structure. When a nerve is severed, the segment downstream from the injury loses its connection to the cell body and begins to degenerate in a process called Wallerian degeneration. Macrophages clear the debris over weeks. The proximal stump, still attached to the spinal cord, is the only side capable of regenerating new nerve endings (axons) and repairing the connection.
Even after the nerve starts trying to heal, regrowth slowly proceeds at roughly one millimeter per day — about an inch a month. This is not a metaphor or an average; it is a biological constant that dictates surgical decision-making and the prognosis for recovery. A nerve injury at the shoulder that needs to reach the hand has months of distance to cover. During that time, the target muscles sit denervated, and they do not wait indefinitely. Motor endplates progressively degrade after denervation, and once that degradation passes a threshold — generally accepted as 12 to 18 months — reinnervation no longer produces meaningful function even if the nerve fibers eventually arrive. This happens on a curve - so with more time comes more permanent loss. The clock is real, and it shapes everything from when surgery is scheduled to whether nerve / tendon transfer is chosen over primary repair.
Microsurgery and Hand Surgery Together
Effective peripheral nerve work requires fluency in two specialties, not one. Hand surgery teaches the biomechanics of the upper extremity — how tendons move, how joints articulate, how the loss of a single nerve translates into specific functional deficits. Microsurgery teaches the technical capacity to operate on structures smaller than a millimeter, under high-magnification microscopes, using sutures finer than a human hair.
Either discipline alone leaves something on the table. A surgeon trained in microsurgery without hand surgery may be able to coapt nerve fascicles beautifully but unable to plan the tendon transfer that will be needed if the nerve repair fails or comes too late. A hand surgeon without microsurgical training may understand the mechanics of the limb but not be able to perform the precision repair that gives the nerve its best chance. The dual training — hand and plastic surgery — is the combination that allows the entire reconstructive ladder to be considered, from primary repair to nerve transfer to functional muscle transfer to prosthetic integration. I draw on both disciplines daily, and my published work spans both — for instance in a book chapter on tendon transfers for low and high ulnar nerve palsy in the third edition of Operative Techniques in Hand and Wrist Surgery, which addresses precisely the situation in which a nerve injury requires a tendon-based solution because timely nerve recovery is no longer possible.
How Nerve Injuries Are Repaired
The right operation depends on the mechanism of injury, the gap between the proximal and distal nerve ends, the time elapsed since the injury, and the function being reconstructed.
Primary Nerve Repair
For sharp, clean transections near the nerve's end — a glass laceration, a knife wound, an iatrogenic cut during surgery — primary neurorrhaphy is the standard. The two ends are aligned and the outer sheath (the epineurium) is sutured under microscopic magnification. The single most important technical principle is tension-free coaptation and capture / retention of the internal nerve fascicles. If the repair is pulled tight, the local blood supply is compromised, scar tissue forms aggressively blocking the nerves healing, and axonal regeneration stalls. When the ends will not come together without tension, primary repair is the wrong operation.
Nerve Grafts and Conduits
When trauma leaves a physical gap, something has to bridge it. The options follow the size of the defect.
For very short gaps in non-critical sensory nerves, a hollow biological or synthetic conduit can guide regenerating axons across the void. For moderate gaps, processed nerve allograft — acellular human nerve tissue that provides the structural scaffolding axons need to migrate — has become a useful tool that avoids the morbidity of harvesting the patient's own nerve. For longer or critical motor reconstructions, autologous nerve graft remains the standard. The sural nerve in the lower leg is the most common donor; it is sensory, expendable, and provides live Schwann cells that actively support regeneration in a way no off-the-shelf product replicates.
Nerve Transfers
Nerve transfers represent one of the more meaningful conceptual changes in the field over the past two decades. Instead of repairing a damaged nerve far proximal to its target — and waiting a year or more for regeneration — an expendable motor nerve branch close to the target muscle is divided and rerouted to power the injured nerve. The distance axons must travel collapses from feet to inches. A multi-year recovery becomes a multi-month recovery. Areas of dense proximal scarring, which often defeat traditional repair, are bypassed entirely. Nerve transfers do not replace primary repair where primary repair is feasible, but in proximal injuries and in delayed presentations they have become the operation that recovers function in patients who would not have recovered otherwise.
Sometimes, nerve transfers are used at the same time as primary repair as a sort of "baby-sitter" to allow the nerve time to reach more distant muscle. This baby-sitter keeps the muscle interested for a longer period of time giving the main nerve a better chance to give meaningful recovery.
Amputation, Neuroma Pain, and the Role of RPNI and TMR
When a major nerve is divided without a target — most commonly after amputation or in cancer ablation surgery — the regenerating axons have nowhere to go. They form a disorganized, hyperexcitable mass called a terminal neuroma. Patients describe sharp electrical pain at the residual limb (tinel sign), persistent phantom sensations, and an inability to wear a prosthetic socket because the pressure on the neuroma is intolerable. Traditional approaches — burying the nerve in muscle or even bone, pulling it back into a less exposed position — gave partial relief by hiding the nerve away or burying it deeper, but did not address why neuromas form or effectively treat the pain stimulus.
Targeted Muscle Reinnervation (TMR) and Regenerative Peripheral Nerve Interfaces (RPNI) take a different approach. Both give the divided nerve a physiologic target - give the nerve a new meaningful job.
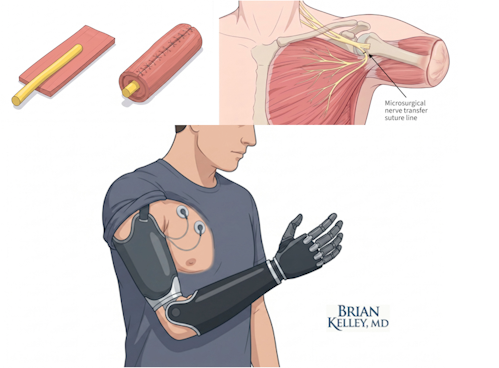
In TMR, the amputated nerve is coapted to a small motor nerve branch entering an expendable segment of muscle near the residual limb. The muscle becomes a destination for the regenerating axons. In RPNI, the amputated nerve is implanted into a small free graft of the patient's own muscle — a neat, contained target that prevents the nerve from forming a neuroma and provides a stable biological signal that can be used downstream. This is different from just putting the nerve into a clump of functioning muscle because in both TMR and RPNI, the muscle needs the nerve as much as the nerve needs the muscle.
The clinical results have changed how I counsel amputation patients. The 2020 multicenter series I co-authored on RPNI for symptomatic hand and digital neuromas — published in Plastic and Reconstructive Surgery — Global Open — examined this technique in a population that historically had limited options, and the work supported RPNI as a useful surgical tool for these difficult cases. My research group has continued to extend this work, including a presentation at the American Society for Peripheral Nerve annual meeting on dermal regenerative peripheral nerve interfaces for neuroma prevention in digit amputation, and a separate ASPN presentation on a modern evidence-based treatment algorithm for peroneal nerve injury. RPNI and TMR are now studied across upper and lower extremity amputations and across both prevention and treatment of neuroma pain, with broadly positive outcomes reported in the literature.
Powering Advanced Myoelectric Prostheses
There is a second purpose to TMR and RPNI beyond pain. Modern myoelectric prostheses — the bionic hands and arms that move in response to muscle signals — read the small electromyographic (EMG) signals generated by muscle contraction. A divided nerve in isolation does not generate enough signal to drive a prosthetic. A muscle that has been reinnervated by that nerve does.
When a patient with TMR or RPNI thinks about closing a hand that is no longer there, the brain still sends the signal down the median or ulnar nerve. That signal now reaches a muscle target. The muscle contracts. Surface electrodes inside the prosthetic socket detect the contraction. The prosthetic finger closes. The biology becomes the amplifier between intention and motion. This is the foundation on which the most advanced prosthetic devices currently in clinical use depend, and it represents one of the more substantive points of contact between modern reconstructive surgery and the field of neuroprosthetics — an area I have addressed in published work on the integration of precision medicine and artificial intelligence into plastic surgery practice.
I was lucky enough to train at the University of Michigan under Paul Cederna, one of the world experts on this technology and have worked with him both surgically and in research on this amazing technology.
Pediatric and Adult Patients: Different Biology, Different Surgery
I treat both children and adults, and the differences between them are not subtle.
Pediatric Patients
Children regenerate nerves faster and remap their cortex more flexibly than adults do. A pediatric brain accommodates a nerve transfer with relative ease — the cortical real estate that controlled the original muscle reorganizes around the new input, often with limited formal therapy required. The anatomical advantage is just as important. A six-year-old's arm is shorter than an adult's, so the same one-millimeter-per-day regeneration covers the distance from injury to target much faster. Conditions that are devastating in adults — obstetric brachial plexus palsy, congenital nerve abnormalities — are often surgically tractable in young children precisely because biology and geometry favor recovery. My published work in pediatric hand surgery includes a first-author qualitative analysis of patient and parent perspectives following reconstruction for congenital hand differences, and a case report on on-top-plasty reconstruction for complicated radial polydactyly, both published in Plastic and Reconstructive Surgery and Hand respectively.
Adult Patients
Adult nerve surgery is dominated by time. The cortex is less plastic, the limbs are longer, and the motor endplates do not wait. A proximal brachial plexus injury in a thirty-year-old motorcycle rider — common in trauma referrals — is a race in which the muscle is degrading on a fixed schedule while the nerve regenerates at a fixed rate. This is the population in whom distal nerve transfers are most important, because they shorten the distance the nerve has to travel and may reach the target before the target is gone. Adult patients also require more deliberate post-operative therapy, both to prevent stiffness and to retrain the brain to use the rewired neuroanatomy.
The decision logic is therefore population-specific. The same injury can warrant primary repair in a child and a distal nerve transfer in an adult, and recognizing why is part of the work.
What the Surgical Process Looks Like for Patients
The path from initial evaluation to final functional recovery is not short, and patients deserve a clear picture of it.
Evaluation begins with a careful history and physical examination, supplemented by electrodiagnostic studies (EMG and nerve conduction studies) that map the deficit, and imaging where indicated. Surgery is then matched to the injury — primary repair, grafting, conduit-assisted repair, nerve transfer, RPNI, TMR, or some combination. The operation itself is typically the shortest part of the journey. After surgery, regeneration takes months. Hand therapy is essential and is not optional. Outcomes are determined by the combination of surgical precision and disciplined rehabilitation, and the patients who do best are the ones who engage with both. Published work from my group has shown that the timing of post-operative hand therapy itself influences outcomes — a reminder that the surgical and rehabilitative components are not separable.
Related Topics
- Peripheral nerve surgery, RPNI, and TMR — overview
- Nerve repair and reconstruction
- Nerve decompression surgery
- TMR and RPNI: What's the Difference?
- RPNI Surgery Recovery Guide
- TMR Guide for Amputees
- Replantation and revascularization
- Breast Sensation After Mastectomy
Medical References
- Hooper RC, Cederna PS, Brown DL, Haase SC, Waljee JF, Egeland BM, Kelley BP, Kung TA. Regenerative Peripheral Nerve Interfaces for the Management of Symptomatic Hand and Digital Neuromas. Plastic and Reconstructive Surgery — Global Open. 2020;8(6):e2792. doi: 10.1097/GOX.0000000000002792. PMID: 32766027.
- Johnson SP, Kelley BP, Waljee JF, Chung KC. Effect of Time to Hand Therapy following Zone II Flexor Tendon Repair. Plastic and Reconstructive Surgery — Global Open. 2020;8(12):e3278. PMID: 33425592.
- Kelley BP, Franzblau LE, Chung KC, Carlozzi N, Waljee JF. Hand Function and Appearance following Reconstruction for Congenital Hand Differences: A Qualitative Analysis of Children and Parents. Plastic and Reconstructive Surgery. 2016;138(1):73e–81e. doi: 10.1097/PRS.0000000000002286. PMID: 27348688.
- Kelley BP, Kubiak C, Chung KC. An On-Top-Plasty Reconstruction for Complicated Radial Polydactyly. Hand. 2018;13(3):NP10–NP13. PMID: 29313380.
- Kelley BP, Chung KC. Soft-Tissue Coverage for Elbow Trauma. Hand Clinics. 2015;43:693–703. PMID: 26498556.
- Kelley BP, Shauver MJ, Chung KC. Management of Acute Postoperative Pain in Hand Surgery: A Systematic Review. Journal of Hand Surgery — American. 2015;40:1610–1619. PMID: 26213198.
- Kim YJ, Kelley BP, et al. Implementing Precision Medicine and Artificial Intelligence in Plastic Surgery: Concepts and Future Prospects. Plastic and Reconstructive Surgery — Global Open. 2019;7(3):e2113. PMID: 31044104.
Book Chapters
- Fujihara Y, Kelley BP, Chung KC, Waljee JF. Tendon Transfers for Low and High Ulnar Nerve Palsy. In: Chung KC (ed): Operative Techniques in Hand and Wrist Surgery, 3rd edition. Elsevier, Philadelphia, PA.
- Kelley BP, Chung KC. Distal Radius Fractures. In: Chung KC (ed): University of Michigan Comprehensive Guide to Upper Extremity Fracture Surgery, 1st edition. Wolters Kluwer Health.
- Kelley BP, Chung KC. Rheumatoid Arthropathies. In: Chung KC (ed): Grabb & Smith's Plastic Surgery, 8th edition. Wolters Kluwer Health.
- Kelley BP. Lower Extremity Reconstruction. In: Brown DL, Levi B (eds): Michigan Manual of Plastic Surgery, 2nd edition. JB Lippincott, Philadelphia, PA.
- Kelley BP. Thoracic and Abdominal Reconstruction. In: Brown DL, Levi B (eds): Michigan Manual of Plastic Surgery, 2nd edition. JB Lippincott, Philadelphia, PA.
Specialty Society Resources
- American Society for Surgery of the Hand — Peripheral Nerve Resources: https://www.assh.org/.
- American Society of Plastic Surgeons — Reconstructive Microsurgery Resources: https://www.plasticsurgery.org/.
- American Society for Peripheral Nerve: https://www.peripheralnerve.org/.
- Dr. Brian P. Kelley faculty profile, Dell Medical School, The University of Texas at Austin; Seton Institute of Reconstructive Plastic Surgery.
Closing Disclaimer
This article is educational and does not establish a doctor-patient relationship. It does not replace individualized consultation, examination, or review of personal medical history and goals. Patients with peripheral nerve injuries, neuroma pain, or amputation-related complications are encouraged to schedule a consultation to review their specific situation and reconstructive options.
Peripheral Nerve SUrgery
FAQs
Frequently Asked Questions
Peripheral nerves regenerate at roughly one millimeter per day, or about one inch per month. The closer the injury is to the target muscle, the sooner functional recovery occurs. Proximal injuries — at the shoulder or upper arm — may take a year or more to demonstrate meaningful recovery in the hand.
RPNI implants a divided nerve into a small free graft of the patient's own muscle, creating a contained physiologic target. TMR coapts the divided nerve to a small motor nerve branch entering a nearby expendable muscle. Both techniques prevent neuroma formation and amplify nerve signals for prosthetic control, but the surgical execution differs.
Both RPNI and TMR can reduce neuroma and phantom limb pain by giving divided nerves a physiologic target rather than allowing them to form a disorganized neuroma. Published outcomes report meaningful pain reduction in many patients, though results vary by injury, prior surgeries, and individual biology.
The surgery itself is performed under anesthesia. Postoperative pain is generally moderate and time-limited. Long-term pain after nerve surgery is more often related to neuroma formation, regenerating axons, or unrelated chronic pain conditions, and is addressed with the combination of medication, hand therapy, and occasionally additional surgery.
Yes, in general. Children have faster regeneration relative to limb length, better cortical neuroplasticity for reorganizing motor and sensory pathways, and better tolerance of the rehabilitation process. Procedures for conditions like obstetric brachial plexus palsy can produce results in infants and young children that would not be biologically possible later in life.
Sharp, clean transections are best repaired within days. Closed or stretch injuries are often observed for several weeks to assess spontaneous recovery before intervention. The outer limit is set by motor endplate viability — generally 12 to 18 months — beyond which reinnervation produces limited functional return regardless of technical success.
Yes. Outcomes after nerve surgery depend on disciplined therapy as much as on surgical precision. Hand therapy maintains range of motion during the regeneration phase, prevents stiffness, and retrains the brain to use rewired neuroanatomy after nerve transfers. Patients who skip therapy generally do not achieve their potential recovery.
A myoelectric prosthesis is not controlled by thought directly — it is controlled by the muscle contractions that thought produces. When a patient with TMR or RPNI thinks about closing the absent hand, the rerouted nerve activates a muscle, and electrodes detect the muscle's electrical signal. The prosthetic finger then closes. The result feels intuitive because the underlying neural pathway is the patient's own.
The Process
Timeline From Consultation to Recovery
01
Consultation
Before consultation, enure any prior studies, operative notes, and imaging are available to our clinic. These might include electromyelography, nerve conduction studies, CT scans, MRIs, functional assessments, physical & occupational therapy assessments, pertinent physican consultations, and operative reports. During this visit, we'll establish our plan and your surgical options if there are any. Care team coordination.
02
Studies or Further Planning
Often, MRI or EMG are not available and may be necessary for operative planning
03
Surgery
If a surgical pathway is chosen, we will plan to schedule. That day often carries an early morning arrival at the hospital. Don't eat anything after midnight. You'll need to coordinate medications that might need to be held prior to surgery in the weeks leading up to our scheduled procedures. Medicines to be held may include anti-coagulation, some diabetes medications, GLP1's (like Ozympic, etc) and others. You may or may not need to stay in the hospital after your procedure.
04
Recovery
Recovery from nerve surgery is often a prolonged endevour. Emotional and physical recovery both take time as your body adjusts to the surgery. Most importantly, we'll stick with you through the entire ordeal.
Nerves may rarely be better right after surgery, for instance, after some decompression surgeries. However, more involved surgeries often see nerve recovery traced out over months or even years. Depending on your options, we'll be able to give you an idea before surgery of what you can expect. Expect to participate in physcial therapy, occupational therapy, or both.
Maximal benefit is often sometime between 1-2 years and almost never results in full restoration of preoperation function. However, we'll work hard to optimize your results and recovery.
Want to learn more?
Book a consultation
