DIEP Flap Breast Reconstruction: A Surgeon's Guide
A surgeon's perspectives on DIEP flap breast reconstruction and a patient's journey to healing.


Written by Brian P. Kelley, MD, Dual Board-Certified Plastic & Hand Surgeon
Affiliate Faculty, Dell Medical School at The University of Texas at Austin
Seton Ascension Institute for Reconstructive Plastic and Hand Surgery, Austin, Texas
Medically reviewed: July 7, 2026 · Last updated: July 7, 2026
Educational content. Not a substitute for individualized medical evaluation.
Introduction
Most patients arrive at a conversation about DIEP flap breast reconstruction during one of the harder weeks of their lives — after a cancer diagnosis, before a prophylactic mastectomy, or years into living with a result they no longer want from a prior reconstruction. The decision is rarely simple, and it deserves precise information rather than reassurance.
A DIEP flap — short for deep inferior epigastric perforator flap — is a microsurgical procedure that rebuilds the breast using the patient's own lower abdominal skin and fat. The tissue is moved with its blood supply intact, sparing the rectus abdominis muscle, and reconnected under the microscope to recipient vessels in the chest. This distinguishes DIEP from the older TRAM flap, which sacrifices muscle, and from implant-based reconstruction, which uses a synthetic device. DIEP flap surgery is one form of autologous breast reconstruction, also called microsurgical breast reconstruction.
This page covers what the procedure is, who is a candidate, how the surgery is performed, what recovery looks like, and what risks should be discussed before consenting. It is written for patients in Austin, Texas, and elsewhere who are weighing options for breast reconstruction after mastectomy.
Is DIEP Flap Breast Reconstruction Right for You?
Candidacy for DIEP flap surgery rests on three pillars: enough abdominal donor tissue, a vascular tree that can support a microsurgical free flap, and a physiology that can tolerate a long operation and a multi-week recovery. None of these is determined by age alone, and none is determined by a single factor.
Body habitus matters, but not in the simple way patients sometimes assume. Patients with very low body mass index may not have enough abdominal tissue to reconstruct a breast of appropriate volume. Patients with high body mass index face elevated risks of wound healing complications and partial flap loss. There is no universal cutoff, and the decision is individualized.
Smoking is a contraindication to elective microsurgical breast reconstruction in most practices. Nicotine constricts the small perforator vessels the flap depends on, and the literature consistently associates active smoking with higher rates of flap loss and donor site complications. Patients are typically asked to stop smoking and all nicotine products well before surgery and to remain off them through the recovery period. I think the truth is that the longer your can be off, the better your outcomes are likely to be.
Prior abdominal surgery is a relative consideration rather than an absolute exclusion. Cesarean section scars, cosmetic surgery, open appendectomy, and prior hernia repair can each affect perforator anatomy. Preoperative CT angiography of the abdominal vessels (CTA) is used at most centers to map perforators before surgery and identify patients in whom the anatomy is unfavorable. Of all of the surgeries likely to affect the DIEP flap the most, tummy tuck robs the body of the exact tissue and vessels use for this operation. Therefore, in patients with tummy tuck history, we may have to be creative with other options to achieve our goals.
Radiation history deserves particular attention. Patients who have already received chest wall radiation, or who are likely to require post-mastectomy radiation, face decisions about timing — immediate versus delayed reconstruction — that affect both flap outcomes and aesthetic results. A systematic review of autologous reconstruction outcomes before and after radiotherapy reported a pooled rate of flap contracture and fibrosis of 27% in flaps exposed to radiotherapy, which is a real consideration when counseling patients about expected aesthetic results in the irradiated setting.
A separate body of work supports immediate autologous reconstruction even when post-mastectomy radiation is anticipated. Review of the literature suggests similar rates of complications and success in autologous breast reconstruction patients exposed to pre- or post-reconstruction radiation, and immediate autologous reconstruction can be considered a viable option even in patients likely to require postmastectomy radiotherapy.
By contrast, in implant-based reconstruction the calculus differs: a parallel systematic review found reconstruction failure rates of approximately 19% and 20% for pre- and post-reconstruction radiation patients, respectively, with similar completion rates of 83% and 80%. These data inform the conversation about why a patient who is likely to need radiation may be steered toward an autologous option. In generally, the ultimate cosmetic outcome is likely to be better in radiated patients with delayed DIEP flap reconstruction. This gives us the advantage of bringing in undamaged skin and tissue to replace the permanently damaged tissues from the chest radiation.
Hormonal therapy is another factor worth raising before surgery. Tamoxifen has been associated with increased rates of thromboembolic events, prompting concerns that it may increase the risk of complications after microvascular breast reconstruction, and a retrospective analysis of 670 patients undergoing delayed microsurgical breast reconstruction found that those receiving tamoxifen within 28 days before reconstruction had a higher rate of immediate total flap loss and a lower rate of flap salvage, but the literature on this question is mixed and continues to evolve.
The decision pathway therefore involves more than a clinic visit. It typically includes preoperative imaging, multidisciplinary coordination with breast oncology, and shared decision-making about timing.
The Surgical Pathway
DIEP flap breast reconstruction is performed under general anesthesia. The patient is positioned supine, with arms tucked or partially abducted depending on whether mastectomy is being performed at the same time. When DIEP is performed immediately, the breast oncology team completes the mastectomy first, preserving the inframammary fold, the pectoralis fascia, and as much of the skin envelope as oncologic safety permits.
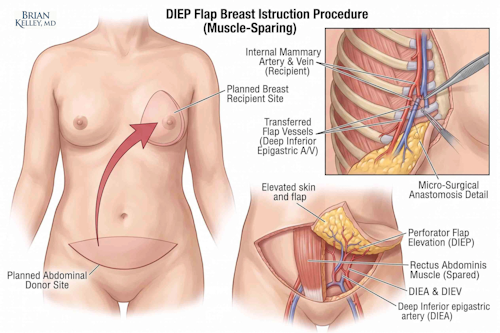
The abdominal portion of the operation begins with a low transverse incision similar in position to an abdominoplasty (tummy tuck) scar. The skin and fat island is elevated off the abdominal wall while individual perforating vessels — branches of the deep inferior epigastric artery and vein — are identified. One or more dominant perforators are selected based on caliber, location, and the perfusion territory they supply. The rectus abdominis muscle is split along its fibers rather than transected, and the pedicle is dissected down to its origin so that adequate length and vessel diameter are obtained. The fascia and the structure of the muscle are preserved, which is the anatomical feature that distinguishes DIEP from a muscle-sacrificing TRAM.
Recipient vessel preparation occurs in parallel. The internal mammary artery and vein are most commonly used; they are exposed through a small window between the costal cartilages. Once both donor and recipient sites are ready, the flap is detached and brought to the chest. Microvascular anastomosis is then performed under the operating microscope using 8-0 or 9-0 nylon sutures (about 2-3x smaller than a typical human hair), joining the artery and vein of the flap to the recipient vessels. After perfusion is confirmed, the flap is shaped and inset to recreate breast volume and contour. At this stage, the priority is safely delivering the new tissue to the breast. Sometimes, for safety, I may choose to leave some contour with plans for future corrections once the flap has taken to it's new home in the breast.
The donor site is closed in layers. Particular attention is paid to the abdominal fascia and to the contour of the closure, since patients are also recovering an abdominal wound and want a presentable result there as well. The belly button is brought through your new abdominal wall and shaped cosmetically. Drains are placed at both the donor site and the chest. Operative duration varies with whether the reconstruction is unilateral or bilateral and whether it is immediate or delayed; patients should expect a long day in the operating room and a 1-3 day admission for flap monitoring. Some surgeons are beginning to allow patients to go home the same day with success, though my patient's typically benefit from the extra help and increased monitoring. This also allows us to react quickly to any challenges should they arise.
For the blood vessels, good caliber veins are likely the most critical component once arterial anatomy is confirmed. Without excellent venous outflow from the flap, patients may be at risk for venous congestion or fat necrosis. This rarely compromises entire flaps, but more commonly small watershed zones of tissue may be affected. That might leave a small firm nodule that can be corrected in a future small operation. To help with blood vessel monitoring, we may use light spectroscopy to monitor hemoglobin and blood flow levels or use implanted doppler devices to listen to the flow to ensure great outcomes. During your stay, I will be monitoring your flap with our nurse and APP teams to make sure your flap and you are doing well.
Post-operatively, we prioritize your pain control. On a pain scale of 0 to 10 - where 10 is the worst thing possible - our goal is never a score of 0. That's not achievable. However, we want you in comfortable recovery - around a 2-3 out of 10. You'll know you're in recovery and you may have some intermittent soreness. However, you won't be in pain all the time. Our goal is to activate you to prepare you for life at home so we will focus on comfort and alertness. I've been lucky enough to be involved in multiple research opportunities focused on pain control after plastic surgery procedures and this has helped to shape my belief in multi-modal pain management to smooth your pathway to discharge and, afterwards, comfort at home.
Recovery Timeline & Realistic Expectations
Recovery from DIEP flap reconstruction unfolds over months, not weeks. The early phase is dominated by flap monitoring; the later phases are about contour, scar maturation, and return to function. The ranges below are typical, not promises. Individual recovery varies with bilateral versus unilateral surgery, immediate versus delayed timing, and prior radiation.
• Hospitalization (typically days 1–4): Patients are admitted, often with intensive flap monitoring during the first 24 to 48 hours. Mobility progresses from sitting to walking. Pain management follows enhanced recovery after surgery (ERAS) principles where applicable, with regional blocks and a stepped-down medication plan to limit opioid exposure. Drain education begins before discharge.
• Weeks 1–2 at home: Activity is restricted. Lifting limits are strict. Sleeping in a slightly upright position is typical. Drain output is recorded and reported. Patients are taught the warning signs that warrant immediate contact with the surgical team — fevers, expanding redness, sudden flap color change, and disproportionate pain. We may discharge you on a blood thinning medication to help reduce risks of deep venous thrombosis (DVT) or clotting issues.
• Weeks 3–6: Most patients begin a gradual return to non-strenuous activity. Driving usually resumes when the patient is off opioid medication and can perform a controlled emergency stop. Return to desk-based work tends to occur earlier than return to physical work; the latter is staged carefully because of donor site healing.
• Months 2–3: Core reconditioning starts under guidance - often with a physical therapy referral. Swelling continues to resolve. Scars enter the active maturation phase. Conversations about a possible second-stage revision — fat grafting for contour, scar revision, or symmetry — typically begin near the end of this window.
• Months 6–12: The aesthetic result reaches near-final form. Optional staged procedures, including nipple-areolar reconstruction, are scheduled if desired. Sensation in the reconstructed breast may continue to evolve for a year or longer.
A note on sensation. Restoration of breast sensibility after reconstruction is an active area of investigation, and patients ask about it frequently. Our systematic review of normal breast sensibility identified that breast sensibility is inversely related to breast volume, but found wide variability across studies in population, breast condition, measurement modality, and anatomic areas measured, with heterogeneity that precluded the generation of normative breast sensibility measurements. The honest answer to "how much sensation will I have?" is that the field does not yet have a normative baseline against which to measure recovery. Some patients regain meaningful sensation; others do not. Promises in either direction are not supported by current evidence.
Risks, Complications, and How They Are Managed
Transparent discussion of risk is part of informed consent. The list below is not exhaustive, and the relative weight of each risk varies by patient. Specific rates from the literature are flagged for verification rather than approximated.
- Flap-specific risks: partial flap loss; total flap loss requiring return to the operating room; venous congestion; arterial thrombosis; fat necrosis (firm, sometimes painful nodules within the flap that may require excision).
- Donor site risks: abdominal bulge; true hernia; seroma; widened or hypertrophic scar; donor site wound healing problems, particularly at the umbilicus or central junction.
- General surgical risks: bleeding, hematoma, infection, deep vein thrombosis, pulmonary embolism, anesthetic complications, pneumothorax, bowel or anatomic injury.
- Reconstruction-specific considerations (but likely not complications): asymmetry between sides; need for revisional surgery; sensory changes; persistent contour irregularities; unsatisfactory aesthetic outcome despite a technically successful flap.
When a flap shows signs of vascular compromise in the early postoperative period, the response is rapid: immediate return to the operating room for exploration and revision of the anastomosis. Salvage is more likely the earlier compromise is identified, which is why monitoring protocols are intensive in the first 24 to 48 hours. This is rare, but we will take it seriously.
Risk in the irradiated setting deserves particular emphasis given the population that most often considers DIEP. The data discussed earlier indicate similar overall complication rates between pre- and post-reconstruction radiation in autologous patients, but a meaningful rate of long-term flap fibrosis and contracture in any irradiated flap. In flap reconstructions exposed to radiotherapy, the pooled rate of flap contracture and fibrosis was 27%. Patients should weigh this when choosing between immediate and delayed reconstruction.
Authority, Affiliations, and Local Context
Dr. Brian P. Kelley is a dual board-certified plastic and hand surgeon practicing in Austin, Texas, with academic Affiliate Faculty at Dell Medical School, at The University of Texas at Austin. He completed medical school at Baylor College of Medicine in Houston, TX and his residency and fellowship training at the University of Michigan. His clinical practice is anchored at Seton Institute of Reconstructive Plastic and Hand Surgery within the Ascension Medical Group, with hospital privileges at Dell Seton Medical Center, Seton Medical Center Austin, and Dell Children's Medical Center. His peer-reviewed publications include systematic reviews on autologous breast reconstruction in the irradiated setting, perioperative considerations in microsurgical reconstruction, and breast reinnervation.
Patients can learn about board-certified standards through the American Society of Plastic Surgeons and the American Board of Plastic Surgery. Internal links to related cluster content: [Breast Cancer Surgery], [Implant-based reconstruction comparison], [Insurance coverage and the Women's Health and Cancer Rights Act].
Related Topics
- DIEP Flap Breast Reconstruction
- Implant-based breast reconstruction
- Autologous Fat Grafting
- Oncoplastic breast reconstruction
- Lymphovenous bypass for breast cancer lymphedema
- Peripheral nerve surgery, RPNI, and TMR
- Breast Sensation After Mastectomy
- TMR and RPNI for nerve pain and amputations
- Direct-to-Implant Breast Reconstruction
- Sex and Intimacy After Breast Cancer
Frequently Asked Questions
Practices vary, and the literature is not uniform. Some centers have implemented protocols to temporarily stop tamoxifen before microvascular breast reconstruction based on concerns about thromboembolic risk and flap complications. The decision should be made jointly by the plastic surgeon and the medical oncologist for each individual patient.
Sensation after DIEP flap reconstruction is variable and incompletely characterized in the literature, even after dedicated nerve restoration procedures. Some patients regain meaningful protective and tactile sensation over a year or more; others have persistent numbness. The literature lacks consistent data delineating normative values for breast sensibility, which limits what any surgeon can promise.
Active smoking does not permanently disqualify you, but it does need to be addressed before surgery. Smoking constricts blood vessels and impairs healing, which raises the risk of mastectomy skin problems, delayed abdominal wound healing, fat necrosis, and, less commonly, flap complications. The encouraging part is that quitting makes a measurable difference. In a large postmastectomy reconstruction study, patients who stopped at least three weeks before surgery had complication rates similar to nonsmokers, while active smokers did significantly worse. Nicotine itself is the vessel constrictor, so vaping and nicotine replacement carry the same concern. For this reason I ask patients to stop smoking and nicotine for a window before and after a DIEP rather than ruling the operation out, and we plan that timing together.
Body type matters, but a higher BMI does not automatically disqualify you. You do need enough lower abdominal tissue to build a breast of the size you want, which is where body type comes in. On safety, the largest multicenter DIEP study (4,561 flaps across 22 centers) found no significant difference in flap loss between normal-weight and obese patients, though obese patients had higher rates of infection and wound healing problems at the donor and breast sites. So elevated BMI raises the risk of complications without ruling out the operation. I assess your abdominal tissue, overall health, and specific risk factors together, and for some patients optimizing weight or health before surgery improves the odds. Very thin patients face the opposite question, whether there is enough tissue, and may be better served by a thigh-based flap.
This is one of the most important timing questions, and the honest answer is that both pathways are reasonable. Radiating a flap can cause fibrosis, some volume loss, and a higher chance of needing a revision, which is why some surgeons prefer to complete radiation first and reconstruct afterward (delayed). But recent data are reassuring for immediate reconstruction. A multicenter cohort comparing immediate versus delayed DIEP reconstruction with post-mastectomy radiation found comparable long-term patient-reported outcomes between the two, despite somewhat more fibrosis and movement restriction reported after immediate reconstruction. The practical approach I often use is a staged one: place a tissue expander to hold the space during radiation, then perform the definitive DIEP after the radiated tissue settles. That preserves the skin envelope while keeping the durable autologous option open. We decide together based on your tumor, your radiation plan, and your priorities. Read more about delayed versus immediate reconstruction on my blog.
Total flap loss, meaning the transferred tissue fails completely and cannot be saved, is uncommon in experienced hands. A German national registry of 3,926 patients reported a total flap loss rate of about 2% and partial flap loss of about 1%, with overall flap success above 97%. A smaller proportion of patients (a few percent) need an urgent return to the operating room in the first day or two to address a blood-clotting problem at the vessel connection, and most of those flaps are successfully saved when caught early, which is why close monitoring after surgery matters. More common than flap loss are minor issues like fat necrosis (firm areas within the flap) and donor-site healing delays, which are usually manageable. Risk rises somewhat with obesity, smoking, and prior abdominal surgery, and I review your individual profile with you.
Most autologous reconstructions involve more than one stage, and this is planned rather than a sign something went wrong. The initial operation builds the breast mound. A second stage, usually a shorter outpatient procedure several months later once the tissue has settled, refines the result. Common refinements include fat grafting to smooth contours or fill small depressions, adjusting symmetry between the two sides, and revising scars. Nipple-areolar reconstruction, when you want it, is typically done at this later stage, after the breast shape has stabilized, using a small local flap to rebuild the nipple followed by tattooing for the areola color. Some patients are content with the mound alone or choose 3D areola tattooing instead. There is no rush on these steps, and we time them to your healing and your goals.
Medical References
The following are peer-reviewed sources cited in this page or directly relevant to the topics discussed:
1. Kelley BP, Ahmed R, Kidwell KM, Kozlow JH, Chung KC, Momoh AO. A systematic review of morbidity associated with autologous breast reconstruction before and after exposure to radiotherapy: are current practices ideal? Annals of Surgical Oncology. 2014;21(5):1732–1738. doi: 10.1245/s10434-014-3494-z. PMID: 24473643.
2. Momoh AO, Ahmed R, Kelley BP, Aliu O, Kidwell KM, Kozlow JH, Chung KC. A systematic review of complications of implant-based breast reconstruction with prereconstruction and postreconstruction radiotherapy. Annals of Surgical Oncology. 2014;21(1):118–124. doi: 10.1245/s10434-013-3284-z. PMID: 24081801.
3. Kelley BP, Valero V, Yi M, Kronowitz SJ. Tamoxifen increases the risk of microvascular flap complications in patients undergoing microvascular breast reconstruction. Plastic and Reconstructive Surgery. 2012;129(2):305–314. doi: 10.1097/PRS.0b013e31823ae86c. PMID: 21987043.
4. Schafer HA, Leathers KO, Mumford KC, Ilangovan S, Vetter IL, Henry SL, Kelley BP, Torres-Guzman RA, Egeland BM. "Toward Breast Reinnervation — What is our Endpoint": A systematic review of normal breast sensibility. Journal of Plastic, Reconstructive & Aesthetic Surgery. 2024;91:383–398. doi: 10.1016/j.bjps.2024.01.057. PMID: 38461623.
5. Dr. Brian P. Kelley faculty profile, Dell Medical School, The University of Texas at Austin; Seton Institute of Reconstructive Plastic Surgery.
6. American Society of Plastic Surgeons — patient resources on breast reconstruction: https://www.plasticsurgery.org/reconstructive-procedures/breast-reconstruction/procedure.
Closing Disclaimer
This article is educational. It does not establish a doctor-patient relationship and does not substitute for an individualized consultation. Surgical candidacy for DIEP flap breast reconstruction is determined only after review of medical history, examination, imaging where indicated, and discussion of personal goals. Patients considering reconstruction are encouraged to schedule a consultation to discuss their specific situation.
Table of Contents
Written By
Want to learn more about breast reconstruction?
The American Society of Plastic Surgeons has many resources to expand your knowledge.



Want to learn more?
Book a consultation
