A Closer Look at Implant-Based Breast Reconstruction
An overview of the history, latest trends, and controversies shaping breast implants and breast reconstruction. Breast Implants and Implant-Based Reconstruction in Austin, TX


Introduction
A breast cancer diagnosis sets in motion a series of decisions, and reconstruction is one of the more personal among them. I practice as a dual board-certified plastic surgeon in Austin, Texas, with Affiliate Faculty appointment at Dell Medical School. Implant-based breast reconstruction is the most commonly performed reconstructive method in the United States, and it is a meaningful part of my practice. The goal of this page is straightforward: to explain how implant reconstruction works, where it fits, where it does not, and what the literature actually says about risks and outcomes.
Patients deserve transparency rather than reassurance. The discussion below covers the history of breast implants — including the regulatory pauses that shape current FDA oversight — the mechanical and biological trade-offs between silicone and saline, the two main surgical pathways, the role of fat grafting in modern reconstruction, and the specific challenge of post-mastectomy radiation. Where the data are mixed, I say so.
Reconstruction Is Not Augmentation
Before discussing techniques, it is worth separating two procedures that share hardware but almost nothing else. Breast augmentation places an implant behind intact native breast tissue or the pectoralis major muscle. The skin envelope is healthy, the blood supply is normal, and the structural support is preserved. Augmentation is an additive operation on a healthy chest wall.
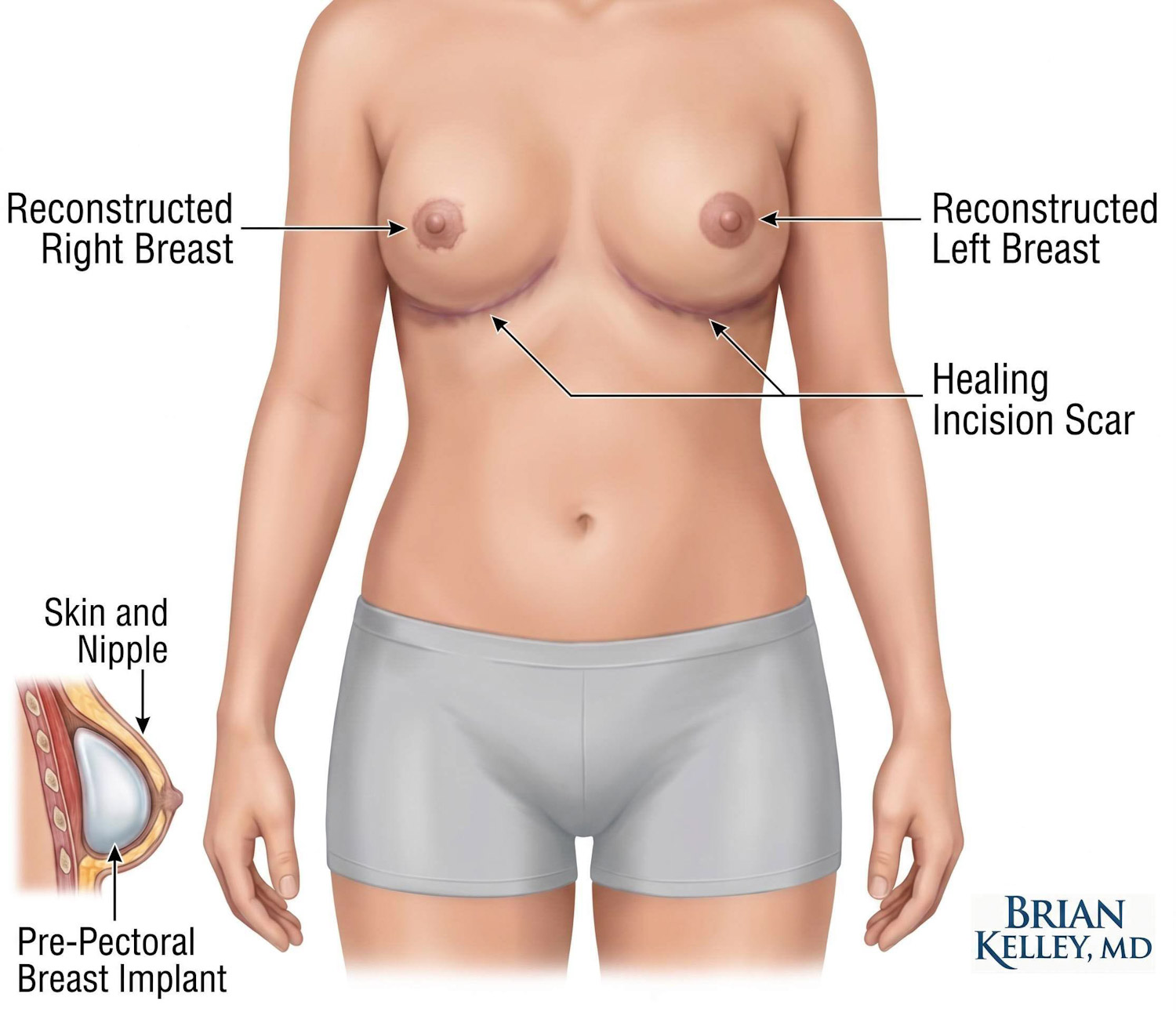
Breast reconstruction follows mastectomy. The breast gland, ductal tissue, and often portions of the overlying skin have been removed to achieve oncologic clearance. What remains is a thin skin envelope, sometimes irradiated, sometimes compromised by prior surgery or comorbidities, with no underlying breast parenchyma. The implant in a reconstructive setting functions as a structural replacement for tissue that is no longer present. It interacts directly with mastectomy skin flaps, the pectoralis muscle, and frequently an acellular dermal matrix (ADM) or synthetic mesh used for support.
This distinction matters because it explains why reconstructive results take more time, more stages, and more revisions than augmentation results. The biomechanics are not the same, and the surgical strategy reflects that.
A Brief History: How We Got Here
Silicone breast implants were introduced in the early 1960s (in Houston, TX at the Baylor College of Medicine), and they represented a substantial advance over the materials that came before. Early devices, however, were not what we use today. Rupture rates were high, and the elastomer shells of first- and second-generation implants permitted "gel bleed" — silicone molecules diffusing through an intact shell into surrounding tissue.
By the late 1980s, anecdotal reports linking silicone implants to autoimmune and connective tissue disorders had accumulated. In 1992, the FDA imposed a moratorium on silicone gel implants for cosmetic use, restricting them to reconstructive patients enrolled in controlled clinical trials. This decision reshaped plastic surgery for over a decade. It also drove the kind of rigorous, longitudinal epidemiological work that the field had previously lacked. This was popularized in the 1997 movie starring Chris Cooper and David Schwimmer, Breast Men wherein the portrayal of plastic surgery and surgeons contributed to the worst perceptions of our field.
Beyond the hype, however, subsequent studies, including the Institute of Medicine's comprehensive review, did not establish a causal link between silicone implants and systemic autoimmune disease. The FDA lifted the moratorium in 2006, approving cohesive-gel silicone implants with strict post-market surveillance requirements. The story did not end there. Regulatory attention has since turned to specific, evidence-based concerns: Breast Implant-Associated Anaplastic Large Cell Lymphoma (BIA-ALCL), squamous cell carcinoma of the implant capsule, and Breast Implant Illness (BII). In 2019, the FDA requested a voluntary recall of Allergan's Biocell textured implants based on their disproportionate association with BIA-ALCL.
The history is worth knowing because it shapes how I counsel patients. Modern devices are safer than their predecessors, but they are not above scrutiny — and the surveillance infrastructure exists precisely because past assumptions did not hold up to data.
Silicone Versus Saline: What the Materials Actually Do
Both modern implant types share a solid silicone elastomer shell. The difference is what fills it.
Saline implants are inserted deflated and filled with sterile saltwater during surgery. Their advantage is rupture safety: if the shell breaches, the saline is absorbed harmlessly by the body and the breast deflates rapidly and visibly. There is no need for routine surveillance imaging. The trade-off is feel and aesthetics. Saline implants tend to be firmer than native tissue and are more prone to visible rippling, particularly in reconstructive patients who lack the subcutaneous fat coverage that augmentation patients usually have. And, if rupture occurs, there is some urgency to replace the implant as scar contracture and collapse of the breast can lead to deformities that are more difficult to correct. Consultation with a surgeon is necessary in these instances.
Silicone gel implants are pre-filled with a highly cross-linked, cohesive gel — sometimes called "gummy bear" implants in lay press. The cohesion means the gel holds its shape even if the shell is damaged. Silicone implants consistently deliver a more natural tactile feel and a more anatomically convincing contour, which is why most reconstructive patients in my practice choose them. Because silicone ruptures are often silent — the breast does not visibly change — the FDA recommends periodic MRI or ultrasound surveillance to detect device failure.
Neither material is perfect. The right choice depends on body habitus, soft tissue coverage, willingness to comply with imaging surveillance, and an individual's aesthetic priorities.
Two Surgical Pathways: Tissue Expander or Direct-to-Implant
Implant reconstruction confines the surgical footprint to the chest wall. There is no abdominal incision, no muscle harvest, no microsurgical anastomosis. The operation is shorter than autologous reconstruction — most cases run one to two hours after completion of the mastectomy — and recovery is faster, with most patients resuming non-strenuous activity within three to four weeks compared to six to eight weeks after a flap procedure. For patients who do not want a second surgical site, who lack adequate donor tissue, or who have other reasons to avoid a long microsurgical case, this is a real advantage.
The execution typically follows one of two pathways.
Two-Stage Tissue Expander Reconstruction
This is the traditional and most widely used approach. At the time of mastectomy, a temporary tissue expander is placed beneath the mastectomy skin envelope. Historically, expanders were placed beneath the pectoralis major muscle (subpectoral). Modern practice increasingly favors pre-pectoral placement — above the muscle — supported by ADM or mesh, which reduces muscle-related pain, animation deformity, and chest tightness.
Over the following weeks to months, the expander is gradually inflated with sterile saline through a small port. The fills happen in clinic and take only a few minutes each. Controlled mechanical stress stretches the skin envelope and induces cellular adaptation, building a pocket large enough to accept the final implant. Once expansion is complete, a second outpatient procedure exchanges the expander for the permanent silicone or saline device. The exchange is shorter and less involved than the initial reconstruction.

Direct-to-Implant Reconstruction
Direct-to-implant reconstruction skips the expansion phase. The permanent implant is placed during the same operation as the mastectomy. The psychological benefit is real: patients wake up with a reconstructed breast mound rather than facing a months-long expansion process. The clinical bar, however, is higher. Direct-to-implant requires excellent mastectomy skin flap viability, favorable preoperative anatomy, and almost always the use of ADM to support the lower pole. Forcing an implant into a tight or marginally perfused skin envelope significantly raises the risk of skin necrosis and reconstructive failure. I reserve direct-to-implant for the patients in whom the criteria genuinely line up.
Fat Grafting: Why Modern Implant Reconstruction Looks Better Than It Used To
One of the most meaningful advances in implant reconstruction over the past fifteen years has been the routine integration of autologous fat grafting. After mastectomy, the skin overlying an implant is thin and lacks the natural soft tissue layer that hides implant edges in cosmetic augmentation patients. The result, particularly at the upper pole and along the medial border of the breast, can be visible rippling, an abrupt step-off where the implant meets native tissue, and a contour that reads as reconstructed rather than natural.
Fat grafting addresses this directly. Adipose tissue is harvested from the abdomen, flanks, or thighs using low-pressure liposuction, processed to remove blood and oil, and injected in microscopic aliquots into the subcutaneous plane over the implant. The graft creates a biological buffer between the device and the skin, smoothing contour irregularities and improving tactile softness. Fat grafting also brings adipose-derived regenerative cells into a tissue bed that often needs them — particularly in irradiated patients, where vascular damage and fibrosis are present and where contour problems are most pronounced.
Fat grafting is rarely a one-time procedure. Most patients who pursue it undergo one or two sessions in the months following the implant exchange. It is an outpatient procedure with limited downtime, and in my experience it is the single technique that most consistently elevates an implant reconstruction from "acceptable" to "natural."

Post-Mastectomy Radiation: The Hardest Decision
The combination of implants and radiation is the most challenging scenario in implant-based reconstruction. Radiation is essential for many breast cancer patients — it reduces local recurrence and improves survival in defined populations — but it does not discriminate between cancer cells and the microvascular network of the chest wall. Irradiated tissue becomes fibrotic, less elastic, and slower to heal. When an implant sits in that environment, the consequences accumulate.
Capsular contracture rates rise. Wound healing problems become more common. Implant exposure and reconstructive failure occur at rates that are not trivial.
In a systematic review I co-authored, my colleagues and I evaluated the published outcomes of implant-based reconstruction in patients exposed to either pre-reconstruction or post-reconstruction radiotherapy. The data were sobering. Reconstruction failure rates — defined as the need to permanently remove the implant — were 19% and 20% for pre- and postreconstruction radiation, respectively. Completion rates were 83% and 80%. In other words, roughly one in five patients undergoing implant reconstruction in the radiated setting will lose the implant.
What this means in practice is that implant reconstruction is not the durable first choice for patients who are likely to require post-mastectomy radiation. When implants are used in that setting, salvage often requires conversion to autologous tissue — using the patient's own well-vascularized tissue to bring blood supply into a damaged field. For some patients, autologous reconstruction (such as a DIEP flap) from the outset is the more durable option. For others, an implant approach combined with staged fat grafting is the right balance. The decision is individualized and is made in conjunction with breast oncology and radiation oncology colleagues.
Risks: What Patients Need to Understand Before Consenting
Transparent risk disclosure is part of informed consent. Implants are medical devices, and they bring a specific set of considerations that autologous tissue does not.
Capsular contracture is the most common long-term complication. The body forms a fibrous capsule around any implant — that is normal. In some patients, the capsule tightens and contracts, distorting the breast and sometimes causing pain. Severe contracture requires surgery to release or remove the capsule and replace the implant.
Infection is uncommon but serious. Strict perioperative antibiotic protocols and surgical technique reduce its incidence, but when infection occurs around an implant it often requires removal of the device, a three- to six-month interval to clear the bacterial load, and a second reconstructive operation later. With autologous reconstruction, the blood supply can bring antibiotics to the problem. With implants, the hardware is secluded from the immune system and biofilm and bacterial biology can conspire to create deep infections requiring implant removal.
Mechanical issues — rupture, malposition, deflation (saline) — are anticipated complications across the lifespan of the device. Implants are not lifetime devices. The FDA estimates a typical device lifespan in the range of 10 to 15 years, and patients should plan on at least one revision over their lifetime.
BIA-ALCL (Breast Implant-Associated Anaplastic Large Cell Lymphoma) is a rare T-cell lymphoma that develops in the fluid and capsule surrounding an implant. It is associated almost exclusively with textured-surface implants, particularly the Allergan Biocell line that the FDA recalled in 2019. Smooth-surface implants, which I use in my practice, carry a substantially lower risk profile. When BIA-ALCL is identified early, it is highly treatable — typically cured by removal of the implant and the surrounding capsule. I my practice, I have never used those textured implants and thankfully none of my patients have been directly affected.
Breast Implant Illness (BII) describes a constellation of systemic symptoms — fatigue, joint pain, cognitive changes — reported by some patients with implants. The FDA recognizes these reports. A clear pathophysiological mechanism has not been established, and research is ongoing. I discuss BII openly with patients during preoperative counseling so that they can weigh the available information for themselves.
Authority, Affiliations, and Local Context
Dr. Brian P. Kelley is a dual board-certified plastic and hand surgeon practicing in Austin, Texas, with academic Affiliate Faculty at Dell Medical School, at The University of Texas at Austin. He completed medical school at Baylor College of Medicine in Houston, TX and his residency and fellowship training at the University of Michigan. His clinical practice is anchored at Seton Institute of Reconstructive Plastic and Hand Surgery within the Ascension Medical Group, with hospital privileges at Dell Seton Medical Center, Seton Medical Center Austin, and Dell Children's Medical Center. His peer-reviewed publications include systematic reviews on autologous breast reconstruction in the irradiated setting, perioperative considerations in microsurgical reconstruction, and breast reinnervation.
Patients can learn about board-certified standards through the American Society of Plastic Surgeons and the American Board of Plastic Surgery. Internal links to related cluster content: [Breast Cancer Surgery], [Implant-based reconstruction comparison], [Insurance coverage and the Women's Health and Cancer Rights Act].
Related Topics
- Implant-based breast reconstruction
- Autologous Fat Grafting
- Oncoplastic breast reconstruction
- Lymphovenous bypass for breast cancer lymphedema
- Peripheral nerve surgery, RPNI, and TMR
- Breast Sensation After Mastectomy
- TMR and RPNI for nerve pain and amputations
- Direct-to-Implant Breast Reconstruction
Written by Brian P. Kelley, MD — Dual Board-Certified Plastic & Hand Surgeon
Medically reviewed: May 4, 2026 · Last updated: May 4, 2026
Educational content. Not a substitute for individualized medical evaluation.
Frequently Asked Questions
No.Breast implants are mechanical devices that wear over time. The FDA estimates atypical lifespan of 10 to 15 years, though some implants last longer withoutissue. Patients should plan for at least one revision surgery over theirlifetime, whether for rupture, capsular contracture, or aesthetic reasons.
Breast reconstruction follows mastectomy and involvesrebuilding a breast where the gland and often skin have been removed. Breastaugmentation places an implant behind intact, healthy native tissue to enhancevolume. The biomechanics, surgical strategy, and complication profiles differsubstantially, even though both procedures use implants.
Yes. MRI is an excellent tool for both breast cancerscreening and evaluating silicone implant integrity. Specific imaging sequencesdistinguish native tissue from silicone gel and can detect silent ruptures.Patients with silicone implants should follow FDA imaging guidance for periodicsurveillance. Tissue expanders, however, may not allow for MRI and thiswould need to be weighed in the risks.
Sensation is significantly altered after mastectomy becausecutaneous nerves are divided during gland removal. Some protective sensationmay return over years, but the reconstructed breast typically remains largelynumb regardless of which reconstructive method is used. Sensate reconstructiontechniques are an active area of research.
A saline implant rupture causes the breast to deflatevisibly over 24 to 48 hours. The sterile saline is absorbed harmlessly by thebody. The implant shell must be surgically removed and replaced. Becauserupture is immediately apparent, saline implants do not require routinesurveillance imaging.
Fat grafting addresses contour irregularities, rippling, andthe visible edges of an implant beneath thin mastectomy skin. It improves thenatural appearance and feel of the reconstruction. Most patients benefit fromone or two staged sessions, and fat grafting is particularly valuable inirradiated patients where soft tissue quality is compromised.
BIA-ALCL is a rare T-cell lymphoma associated almostexclusively with textured-surface implants. The FDA requested a voluntaryrecall of Allergan Biocell textured implants in 2019 because of theirdisproportionate association with this disease. Smooth-surface implants, whichI use in my practice, carry a substantially lower risk profile.
Medical References
- Momoh AO, Ahmed R, Kelley BP, Aliu O, Kidwell KM, Kozlow JH, Chung KC. A systematic review of complications of implant-based breast reconstruction with prereconstruction and postreconstruction radiotherapy. Annals of Surgical Oncology. 2014;21(1):118–124. doi: 10.1245/s10434-013-3284-z. PMID: 24081801.
- American Society of Plastic Surgeons. Breast Reconstruction Options. https://www.plasticsurgery.org/reconstructive-procedures/breast-reconstruction.
- American Society of Plastic Surgeons. BIA-ALCL Resources. https://www.plasticsurgery.org/patient-safety/bia-alcl-summary.
- U.S. Food and Drug Administration. Breast Implants — Risks and Complications. https://www.fda.gov/medical-devices/breast-implants/risks-and-complications-breast-implants.
- U.S. Food and Drug Administration. FDA Requests Allergan Voluntarily Recall Natrelle BIOCELL Textured Breast Implants. July 24, 2019.
- The New York Times. "Silicone Breast Implants Approved by F.D.A." November 18, 2006. — Coverage of the FDA's decision to lift the silicone gel implant moratorium.
- The Wall Street Journal. "FDA Asks Allergan to Recall Some Textured Breast Implants Tied to Cancer." July 24, 2019. — Coverage of the Biocell recall and BIA-ALCL.
- The New York Times. "What to Know About Breast Implant Illness." Reporting on BII symptoms, FDA labeling changes, and ongoing research. [INSERT VERIFIED URL].
- Dr. Brian P. Kelley faculty profile, Dell Medical School, The University of Texas at Austin; Seton Institute of Reconstructive Plastic Surgery.
Closing Disclaimer
This article is educational and does not establish a doctor-patient relationship. It is not a substitute for individualized consultation, examination, or review of personal medical history and oncologic treatment plans. Patients considering breast reconstruction are encouraged to schedule a consultation to discuss their specific situation and reconstructive options.



Want to learn more?
Book a consultation
