Implant-Based Breast Reconstruction
Achieve natural-looking results with less invasive procedures using advanced silicone and saline implant techniques. We provide personalized options, including immediate, staged, and direct-to-implant solutions.

What is implant-based breast reconstruction?
Implant-based breast reconstruction is the most commonly performed method of restoring breast volume after mastectomy in the United States. As a dual board-certified plastic surgeon in Austin, Texas, implant-based breast reconstruction represents a significant portion of the reconstructive work I do. Patients often choose this option for specific reasons: it avoids a separate donor site, requires a shorter operation, and allows a faster return to baseline activity compared to autologous tissue transfer. But it also carries its own set of considerations — device longevity, infection, capsular contracture, and the impact of radiation on implant success.
The goal of this page is to explain how implant-based breast reconstruction works, who it suits, and what the decision involves. The information is drawn from peer-reviewed literature and clinical practice, including systematic reviews I co-authored on reconstruction outcomes in the setting of radiation therapy.
Two Surgical Approaches: Tissue Expander vs. Direct-to-Implant
Implant reconstruction generally follows one of two pathways. The first is a two-stage tissue expander approach. The second is single-stage direct-to-implant reconstruction. The choice depends on the quality of the mastectomy skin flaps, the volume of breast being reconstructed (and maybe more importantly, the volume desired), and whether the mastectomy is immediate or delayed.
Why are tissue expanders used?
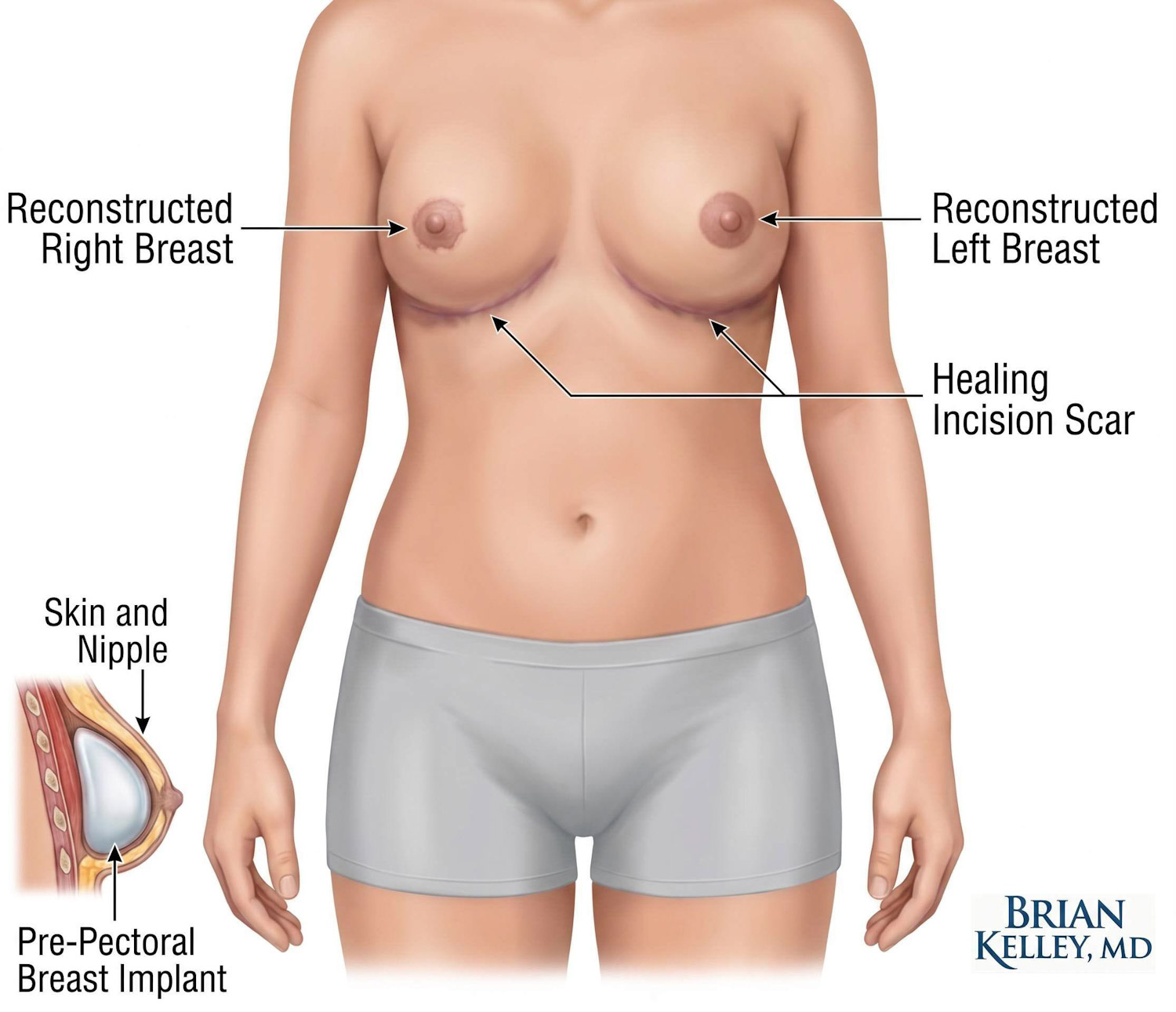
The two-stage approach is the traditional and most common method. The main purpose of this method is that it saves all options and helps to prepare the skin and remaining tissues for the final reconstruction, often given back tissue laxity that an implant alone can't provide. At the time of mastectomy, a temporary tissue expander is placed beneath the skin envelope. Historically, tissue expanders were placed under the pectoralis major muscle, but now they're often positioned above it using acellular dermal matrix or synthetic mesh. This technique preserves muscle function and reduces pain and deformity.
Over the following weeks to months, the expander is gradually filled with sterile saline through a small port, either magnetic or palpable beneath the skin. This controlled inflation stretches the overlying skin and soft tissue, creating a pocket that can accommodate the final implant. The fills are performed in the office and take just a few minutes. The injections are almost always painless since nerves are often disrupted and not recovered after the mastectomy. Once the tissue envelope reaches the desired size, a second outpatient procedure is scheduled to remove the expander and exchange it for a permanent silicone or saline implant. This exchange surgery is shorter and less involved than the initial reconstruction.

Can I go direct-to-implant for my reconstruction?
Direct-to-implant reconstruction skips the expansion phase. During a single operation, the permanent implant is placed immediately after the mastectomy is completed. This approach works best when the mastectomy preserves healthy, well-perfused skin flaps with enough laxity to accommodate the implant without tension. It is most often used in prophylactic mastectomies or smaller-volume reconstructions where the native skin envelope is adequate. Direct-to-implant is faster and can eliminate the need for a second exchange surgery, but patient selection is critical — forcing an implant into a tight or compromised skin envelope significantly raises the risk of complications like mastectomy flap necrosis.
What's the difference between silicone and saline breast implants?
Breast implants are filled with either silicone gel or saline. The choice affects the feel of the reconstructed breast, the size of the surgical incision, and the surveillance required over time.
Silicone gel implants are pre-filled at the factory and come in a range of volumes and profiles. Modern silicone is highly cohesive, meaning the gel holds its shape even if the outer shell is damaged. Cohesive gel implants feel closer to natural breast tissue and drape more naturally than saline. The downside is that a silicone implant requires a slightly larger incision to insert, and because rupture is often silent — meaning the breast does not visibly deflate — the FDA recommends periodic imaging surveillance with MRI or ultrasound to detect leaks. I often use Allergan or Motiva style implants in my practice for their favorable complication rates.
Saline implants are inserted deflated and filled with sterile saltwater once in position. This allows for smaller incisions and precise volume adjustments during surgery. If a saline implant ruptures, the breast deflates rapidly and the problem is immediately obvious. The body safely absorbs the saline. The trade-off is that saline implants tend to feel firmer and may show visible rippling, particularly in thin patients with minimal soft tissue coverage.
In my practice, most patients undergoing breast reconstruction opt for silicone implants because of the more natural feel and appearance. The choice is individualized based on patient preference, body habitus, and willingness to comply with long-term imaging recommendations.
What are the advantages of implant-based breast reconstruction over autologous?
The primary appeal of implant-based reconstruction is simplicity. There is no need to harvest tissue from another part of the body. This means no abdominal incision, no donor site healing, no sacrifice of muscle, and no extended recovery from a microsurgical procedure. The operation is shorter — tissue expander placement typically takes one to two hours — and postoperative recovery is measured in weeks rather than months. Most patients return to non-strenuous activity within three to four weeks, compared to the six to eight weeks typical after autologous reconstruction.
For patients who want breast reconstruction but are not candidates for a long microsurgical case, who do not have adequate donor tissue, or who simply prefer to avoid donor site morbidity, implants are a reasonable and widely used option.
What are the risks with implant-based breast reconstruction?
Implants are medical devices, not living tissue. The body recognizes them as foreign and forms a fibrous capsule around the implant as part of the normal healing process. In some patients, this capsule tightens excessively — a condition called capsular contracture. Severe capsular contracture distorts the shape of the breast and can cause pain. When this occurs, surgical intervention is required to release the scar tissue and replace the implant.
Other risks include infection, hematoma (blood collection), seroma (fluid collection), implant malposition, and mechanical rupture. Implants are not lifetime devices. They do not integrate biologically with the body's vascular system, and over time the risk of issues increases. Revision surgery at some point in a patient's life is statistically likely, whether for contracture, rupture, or aesthetic revision.
The decision to proceed with implant reconstruction should be made with the understanding that implants require long-term monitoring and that future surgery is possible.

What changes after radiation if I want implant-based breast reconstruction?
Post-mastectomy radiation therapy significantly alters the risk profile of implant-based reconstruction. Radiation induces progressive tissue fibrosis, damages small blood vessels, and compromises the elasticity and healing capacity of the skin. When a synthetic implant is placed in an irradiated field, complication rates rise substantially.
A systematic review I co-authored examined outcomes in patients who underwent implant reconstruction with either pre-reconstruction or post-reconstruction radiation. Reconstruction failure rates — defined as the need to remove the implant permanently — were 19% and 20% for pre- and postreconstruction radiation, respectively. Completion rates were 83% and 80%. These are not trivial numbers. They mean that roughly one in five patients who receive radiation in the setting of implant reconstruction will experience implant failure requiring removal.
When an implant fails in the radiated setting, salvage typically requires conversion to autologous tissue reconstruction — using the patient's own tissue to bring healthy, vascularized coverage to the irradiated area. For patients who are likely to require post-mastectomy radiation, autologous reconstruction is often the more durable first choice. When implant reconstruction is chosen despite radiation, patients should be counseled on the elevated risk of contracture, poor aesthetic outcomes, and potential need for secondary surgery.
Does the FDA recommend surveillance?
Breast implants have a complex regulatory history. In 1992, the FDA restricted silicone gel implants to reconstructive use only, citing concerns about a possible link to autoimmune disease. For more than a decade, silicone implants were available for breast reconstruction patients but not for cosmetic augmentation. The restriction was lifted in 2006 after extensive epidemiological studies found no causal relationship between silicone implants and systemic autoimmune or connective tissue disorders.
Current FDA oversight focuses on two specific issues. The first is Breast Implant-Associated Anaplastic Large Cell Lymphoma (BIA-ALCL), a rare T-cell lymphoma linked primarily to textured-surface implants. To minimize this risk, I use smooth-surface implants in my practice. The second is Breast Implant Illness (BII), a term used to describe a constellation of systemic symptoms — fatigue, joint pain, cognitive difficulty — reported by some patients with implants. The FDA recognizes these reports, but a clear pathophysiological mechanism has not been established. Research is ongoing.
Patients considering implant reconstruction receive comprehensive counseling on these issues, the need for long-term surveillance imaging for silicone implants, and the signs of potential complications that warrant immediate evaluation.
What is "fat grafting" and why might I need it if I get implant-based breast reconstruction?
Autologous fat grafting is an indispensable adjunct procedure utilized extensively in both implant-based and autologous reconstructions. This specialized technique involves harvesting fat via low-pressure liposuction from donor areas such as the flanks, thighs, or abdomen. The harvested fat cells are then purified and strategically injected in small, precise aliquots into the reconstructed breast. Fat grafting is essential for refining topographical contours, filling minor depressions or step-offs, correcting mild asymmetry, and optimizing the final aesthetic result to perfectly mimic the natural slope and projection of the native breast. It is particularly effective and important in patients with a history of radiation treatment.

What is the timeline for breast reconstruction with implants?
The decision to undergo implant-based breast reconstruction requires thorough, highly individualized preoperative planning. The initial consultation involves a meticulous review of the patient's oncologic history, anatomical suitability, and personal reconstructive goals.
The operative procedure itself is much more simple that autlogous microsurgical breast reconstruction with faster recovery and lower donor site morbidity. However, there are significant maintanence trade-offs and the risks with regard to infection, capsular contracture, or post-mastectomy radiation failure are real. Postoperative care may require an overnight hospital stay thought many patients go home the same day. Total recovery, enabling a full return to all baseline physical activities and rigorous exercise, generally spans four to eight weeks in most patients and may require physical therapy consultation.
What are likely outcomes?
Achieving excellence in breast reconstruction requires technical mastery, extensive operative experience, and an unwavering commitment to patient safety and long-term oncologic health. The intersection of an active clinical practice in Austin and ongoing academic research facilitates a surgical environment where safety protocols, aesthetic outcomes, and patient education are continuously optimized.
Written by Brian P. Kelley, MD — Dual Board-Certified Plastic & Hand Surgeon
Medically reviewed: May 4, 2026 · Last updated: May 4, 2026
Educational content. Not a substitute for individualized medical evaluation.
Related Topics
- Blog Post on Implant-based breast reconstruction
- Oncoplastic breast reconstruction
- Post-Mastectomy Breast Sensation
- Autologous Fat Grafting
- Lymphovenous Bypass and Lymphedema Prevention
- Facial and Mohs reconstruction
- Extremity reconstruction and limb salvage
- Lymphovenous Bypass for Post-Mastectomy Lymphedema
Closing Disclaimer
This article is educational and does not establish a doctor-patient relationship. It does not replace individualized consultation, examination, or review of personal medical history. Patients with sensory changes or pain after mastectomy are encouraged to discuss their specific situation with their oncology team and, when appropriate, with a plastic surgeon experienced in nerve and breast surgery.
Want to learn more?
Book a consultation
