Targeted Muscle Reinnervation (TMR) and Regenerative Peripheral Nerve Interface (RPNI)
Advanced nerve surgery techniques for effective pain mitigation and enhanced prosthetic control in amputees.
Introduction
Targeted Muscle Reinnervation (TMR) and Regenerative Peripheral Nerve Interfaces (RPNI) are two related microsurgical procedures that have changed the management of nerve pain after amputation, the prevention of post-surgical neuromas, and the integration of advanced prosthetic devices with the human body. Both procedures answer the same biological problem: when a nerve is divided and has no target, it forms a disorganized, hyperexcitable mass of regenerating axons — a neuroma — that produces pain and prevents comfortable use of a prosthetic. TMR and RPNI give the divided nerve somewhere to go.
I practice as a dual board-certified plastic and hand surgeon in Austin, Texas, with Affiliate Faculty appointments at Dell Medical School and a partner in the Seton Institute for Reconstructive Plastic and Hand Surgery. Neuroma surgery and RPNI are part of my published research, including a multicenter series in Plastic and Reconstructive Surgery — Global Open and presentations at the American Society for Peripheral Nerve. This page describes both procedures, their indications, their outcomes, and the broader contexts — including post-mastectomy pain — in which similar principles apply.
For broader peripheral nerve content including pediatric versus adult considerations and the underlying biology of nerve regeneration, see the [peripheral nerve surgery page]. For the surgical management of established neuromas in non-amputation contexts, see the [nerve repair and reconstruction page].
The Problem These Procedures Solve
A peripheral nerve that is divided needs a target. In the normal anatomy, motor nerves end at neuromuscular junctions in muscle, and sensory nerves end at receptors in skin and other tissues. When trauma, surgery, or amputation severs a nerve and removes its target, the proximal stump still attempts to regenerate — that is what nerve tissue does. With no destination, the regenerating axons form a disorganized cluster called a terminal neuroma. In other words - the nerve needs a job!
Terminal neuromas produce two clinical problems. The first is pain. A neuroma at the end of a divided nerve is hyperexcitable; it generates spontaneous and provoked discharges that the brain interprets as sharp, electrical, or burning pain in the distribution of the original nerve. The second, in amputees, is functional. The neuroma sits where the residual limb meets a prosthetic socket, and the pressure of the socket against the neuroma is intolerable. Many amputees who would otherwise benefit from a prosthetic cannot wear one because of this.
Older surgical approaches — burying the nerve in muscle, traction neurectomy, transposing the nerve away from pressure points — were palliative rather than physiologic. They did not address why neuromas form. TMR and RPNI do.
Targeted Muscle Reinnervation (TMR)
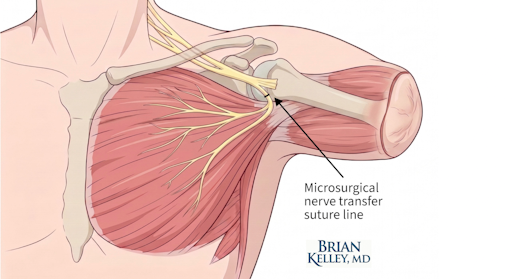
TMR coapts the divided nerve to a small motor nerve branch entering an expendable segment of muscle near the amputation or division site. The procedure is performed under microscopic magnification. The motor nerve branch supplying the target muscle is divided, and the larger amputated nerve is sutured end-to-end to the smaller motor branch. The amputated nerve's regenerating axons then grow into the existing motor nerve pathway and reinnervate the muscle, which becomes their new functional target.
TMR was developed initially as a strategy to enable myoelectric prosthetic control after major upper extremity amputation. The clinical observation that TMR also reduced neuroma pain emerged from those early experiences and has since been confirmed in multiple series. TMR is now offered both at the time of amputation as a preventive measure and as a treatment for established symptomatic neuromas in patients who underwent amputation without it.
Regenerative Peripheral Nerve Interface (RPNI)
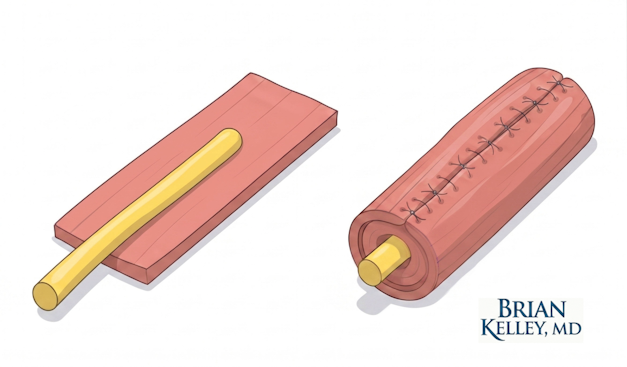
RPNI takes a different approach. Rather than coapting the divided nerve to a motor nerve branch in an existing muscle, RPNI implants the divided nerve into a small free graft of the patient's own skeletal muscle. The graft, typically a few centimeters long and less than a centimeter wide, is harvested from a nearby muscle. The end of the divided nerve is wrapped in the muscle graft and secured with sutures.
The biology that follows is the key to the procedure. The free muscle graft initially survives by diffusion, then becomes revascularized from the surrounding tissue. The implanted nerve sprouts axons into the graft and reinnervates it, generating a new neuromuscular junction system contained within the graft. The result is a self-contained, well-organized target that prevents the disorganized neuroma formation that would otherwise occur, and that generates a stable electrical signal when the nerve is activated.
RPNI has both prophylactic and therapeutic applications. As a prophylactic measure at the time of amputation, RPNI is performed on the divided nerves to prevent neuroma formation before it occurs. As a therapeutic procedure, it is offered to patients with established symptomatic neuromas — the existing neuroma is excised, and the freshened nerve end is implanted in a new muscle graft.
My published work in this area includes the 2020 multicenter series in Plastic and Reconstructive Surgery — Global Open on RPNI for symptomatic hand and digital neuromas, which examined the technique in a population of patients who had already developed painful neuromas. Earlier work from the same collaborative was presented at the American Society of Plastic Surgeons. My research group at Dell has also presented at the American Society for Peripheral Nerve on novel use of dermal RPNI for neuroma prevention in digit amputation, extending the technique to a specific clinical scenario in which conventional approaches have been less effective.
Comparing TMR and RPNI
The two procedures address the same biology through different surgical approaches. TMR uses an existing muscle as the target by intercepting its motor nerve supply. RPNI creates a new target by harvesting a small muscle graft and implanting the nerve into it. Both work. The choice between them depends on the anatomy at the operative site, the size and number of nerves to be addressed, the surgeon's familiarity with each technique, and the specific clinical goals.
In practice, TMR is often selected for major proximal amputations where multiple large nerves need targets and where existing motor nerve branches in expendable muscles are conveniently located. RPNI is often selected for smaller nerves, for digit amputations, for revision procedures on established neuromas, and for situations in which a contained, controllable target is preferable. Many surgeons use both techniques in the same patient when the clinical situation calls for it.
Powering Advanced Myoelectric Prostheses
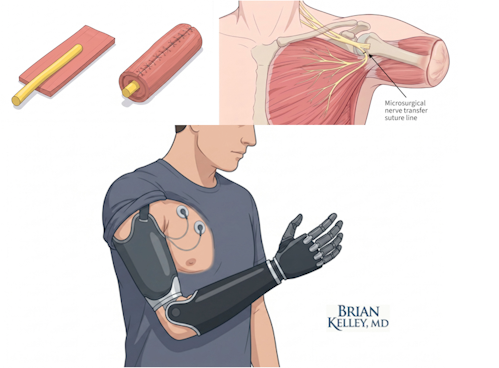
A second purpose of TMR and RPNI, beyond pain management, is enabling intuitive control of advanced myoelectric prosthetic devices. The biological principle is the same. When a patient with a major upper extremity amputation thinks about closing the absent hand, the brain still sends the motor signal down the median or ulnar nerve. In the conventional anatomy, that signal reaches no functional target. After TMR or RPNI, that signal reaches a muscle target — the reinnervated muscle in TMR, the implanted muscle graft in RPNI. The muscle contracts in response.
Surface electrodes inside the prosthetic socket detect the muscle's electromyographic (EMG) signal. The prosthetic interprets the signal and moves accordingly — closing a hand, flexing an elbow, rotating a wrist. The control feels intuitive to the patient because the underlying neural pathway is the patient's own. The biological tissue functions as an amplifier, converting the small electrical signal of a divided nerve into the larger and more readily detectable signal of muscle contraction.
This integration is the foundation of the most advanced upper extremity prosthetic devices currently in clinical use. The work sits at the boundary between reconstructive surgery and neuroprosthetics, and it is one of the more substantive points of contact between modern hand surgery and the technology field.
The Broader Context: Post-Surgical Pain Beyond Amputation
The principles that drove the development of TMR and RPNI apply beyond major limb amputation. Any surgical procedure that divides a peripheral nerve creates the potential for neuroma formation and chronic pain. Two contexts deserve particular mention.
Post-mastectomy pain. Mastectomy divides multiple sensory nerves of the chest wall, and a substantial fraction of patients develop chronic pain after mastectomy that has features consistent with neuroma formation in the chest wall and axilla. The 2024 systematic review I co-authored as senior author in the Journal of Plastic, Reconstructive & Aesthetic Surgery — "Toward Breast Reinnervation: What is Our Endpoint" — examined breast sensibility after mastectomy and reconstruction, including the methodology of measuring sensory recovery. The clinical implication, for surgeons working at the intersection of breast reconstruction and nerve management, is that nerve handling at the time of mastectomy and reconstruction has consequences that may extend years beyond the initial operation. Techniques analogous to TMR and RPNI — and dedicated breast reinnervation approaches — are an area of active investigation for both pain prevention and sensory restoration.
Other post-surgical neuromas. Patients can develop symptomatic neuromas after a wide range of operations, including hernia repair, abdominal surgery, foot and ankle surgery, and oncologic resections that divide identifiable peripheral nerves. The same surgical principles — providing a divided nerve with a physiologic target rather than allowing it to form a disorganized neuroma — apply, and TMR or RPNI can be considered in selected cases.
Outcomes
The published outcomes literature for TMR and RPNI is favorable but not uniform. Across multiple series, both techniques produce meaningful reductions in neuroma pain and phantom limb pain in many patients, with response rates that compare favorably to older approaches. Outcomes are better when the procedures are performed prophylactically at the time of amputation than when they are performed for established neuromas, though both indications are supported by the literature.
For patients seeking myoelectric prosthetic control, TMR and RPNI improve the quality of EMG signaling in the residual limb and enable control schemes that would not be possible without them. The functional results depend on the prosthetic technology, the rehabilitation, and the patient's engagement with the training process — but the biological foundation that the surgery creates is what makes the rest possible.
The work is not a guarantee. Some patients have residual pain after TMR or RPNI. Some patients with severe long-standing neuromas do not achieve full relief. Selection, expectations, and counseling matter as much in this work as they do in any other area of nerve surgery.
Risks
The risks of TMR and RPNI overlap with those of any peripheral nerve operation: bleeding, infection, persistent or recurrent pain, scarring around the surgical site, incomplete relief of symptoms, and the rare possibility of new pain at the operative site. The donor site for RPNI muscle grafts produces a small permanent change in the donor muscle, generally without functional consequence. Patients who elect either procedure should expect a post-operative recovery period before the biological reorganization is complete and before the benefits of the operation are fully realized.
Written by Brian P. Kelley, MD — Dual Board-Certified Plastic & Hand Surgeon Medically reviewed: May 4, 2026 · Last updated: May 4, 2026 Educational content. Not a substitute for individualized medical evaluation.
Frequently Asked Questions
Medical References
- Hooper RC, Cederna PS, Brown DL, Haase SC, Waljee JF, Egeland BM, Kelley BP, Kung TA. Regenerative Peripheral Nerve Interfaces for the Management of Symptomatic Hand and Digital Neuromas. Plastic and Reconstructive Surgery — Global Open. 2020;8(6):e2792. PMID: 32766027.
- Hart SE, Hooper RC, Cederna PS, et al. Regenerative Peripheral Nerve Interfaces for the Management of Symptomatic Hand and Digital Neuromas. Plastic and Reconstructive Surgery — Global Open. 2020;8(4 Suppl):6–7.
- Bashour L, Schafer H, Kelley BP. Novel Use of Dermal Regenerative Peripheral Nerve Interfaces for Neuroma Prevention in Digit Amputation. ePoster, American Society for Peripheral Nerve, Annual Meeting, January 2021.
- Schafer HA, Leathers KO, Mumford KC, Ilangovan S, Vetter IL, Henry SL, Kelley BP, Torres-Guzman RA, Egeland BM. "Toward Breast Reinnervation — What is our Endpoint": A Systematic Review of Normal Breast Sensibility. Journal of Plastic, Reconstructive & Aesthetic Surgery. 2024;91:383–398. PMID: 38461623.
- American Society for Peripheral Nerve: https://www.peripheralnerve.org/.
- American Society for Surgery of the Hand: https://www.assh.org/.
Related Topics
- Peripheral nerve surgery, RPNI, and TMR — overview
- Nerve repair and reconstruction
- Nerve and Tendon Transfers
- Carpal Tunnel & Nerve decompression surgery
- Replantation and revascularization
- TMR for Amputees: A guide
- TMR vs RPNI: What's the Difference?
- RPNI Recovery Guide
Closing Disclaimer
This article is educational and does not establish a doctor-patient relationship. It does not replace individualized consultation, examination, or review of personal medical history. Patients with neuroma pain, phantom limb pain, or amputation-related concerns are encouraged to schedule a consultation to discuss their specific situation and reconstructive options.
TMR and RPNI Surgery
FAQs
Frequently Asked Questions
TMR coapts a divided nerve to a motor nerve branch in an existing muscle, redirecting the regenerating axons into the existing neuromuscular pathway. RPNI implants the divided nerve into a small free graft of muscle, creating a contained physiologic target. Both prevent neuroma formation and amplify nerve signals for prosthetic use; the surgical execution differs.
Both techniques can reduce phantom limb and residual limb pain in many patients, with published outcomes showing meaningful improvement across multiple series. We should not expect them to eliminate pain entirely. Patients with severe long-standing neuromas, multiple prior surgeries, centrally reinforced pain feedback, spinal cord or root avulsion injuries, or other chronic pain contributors may experience partial or minimal pain relief rather than complete relief.
Both procedures can be performed prophylactically at the time of amputation to prevent neuroma formation, or therapeutically months to years later for patients who developed symptomatic neuromas. Outcomes are generally better when the procedures are performed prophylactically, though delayed treatment of established neuromas remains worthwhile in selected patients.
Both procedures can improve myoelectric prosthetic control by amplifying the EMG signals available in the residual limb. The functional improvement depends on the prosthetic device, the rehabilitation, and the level of amputation. Patients with major upper extremity amputations seeking to use advanced multifunction prostheses often benefit substantially.
Yes. Patients who underwent amputation without TMR or RPNI and who later develop symptomatic neuromas can be evaluated for delayed treatment. The existing neuroma is typically excised at the time of the new procedure, and the freshened nerve end is then managed with TMR or RPNI. Outcomes may be worse than if the operation was performed right away but can still be good.
Want to learn more?
Book a consultation
