Nerve Repair and Reconstruction in Austin, TX
Comprehensive nerve repair solutions for enhanced hand and wrist recovery.

Introduction
Nerve repair is among the most technically demanding work in hand surgery, and the most consequential. A nerve repair done well can restore sensation to a fingertip or movement to a paralyzed muscle. A nerve repair done late, under tension, or with the wrong technique often produces a result that can leave the patient and the surgeon both disappointed. This is further complicated by innate physiology of nerves - sometimes precluding outcomes despite best efforts. This page describes the principles that govern when and how nerves are repaired, what the patient should expect from each technique, and what realistic outcomes look like.
For broader peripheral nerve content — including nerve transfers, Regenerative Peripheral Nerve Interfaces (RPNI), Targeted Muscle Reinnervation (TMR), and pediatric versus adult considerations — see the [peripheral nerve surgery page]. This page focuses specifically on the repair and reconstruction of injured nerves.
When Nerves Are Repaired
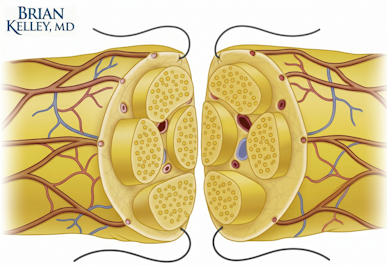
Sharp lacerations are repaired early when feasible. A clean transection of a digital nerve from a glass laceration, a knife wound, or an iatrogenic injury during another operation is best repaired primarily — meaning end-to-end coaptation (sewing two nerve endings together) under the microscope, performed within days of the injury. The proximal stump retains its capacity to regenerate axons - the sprouting nerve endings that grow away from the spinal cord; the distal segment provides the structural pathway but is no longer actually nerve tissue. Bringing the two ends together promptly, without tension and with accurate fascicular alignment, gives the repair its best chance.
When primary repair is not feasible — because the wound is contaminated, because the patient is unstable, because the nerve injury is missed at the initial evaluation, or because tissue conditions do not permit definitive surgery — secondary repair is performed once conditions allow. Secondary repair is technically more difficult than primary repair. The retracted nerve ends often cannot be brought together without tension, the proximal stump may have formed a neuroma, and scar tissue obscures the working field. The longer the delay, the more likely it is that the repair will require a graft or a transfer rather than a direct end-to-end coaptation.
The biological deadline matters as much as the surgical timing. Peripheral nerves regenerate at roughly one millimeter per day, and motor endplates in denervated muscle progressively degrade after denervation. Once that degradation passes a threshold — generally accepted as 12 to 18 months — reinnervation does not produce meaningful muscle function even if the nerve fibers eventually arrive. This is the single most important constraint on nerve surgery decision-making.
Direct Repair (Primary Neurorrhaphy)
Direct repair is the standard for sharp transections that can be brought together without tension. The operation is performed under microscopic magnification. The epineurium — the outer connective tissue sheath of the nerve — is approximated with fine sutures, typically 8-0 to 10-0 caliber (2-3 times more narrow than a human hair). Internal fascicular alignment is judged by the visible pattern of the nerve ends and by knowledge of the local anatomy. The single most important technical principle is tension-free coaptation. A repair pulled tight constricts its own blood supply, generates aggressive scar formation, and impedes the very axonal regeneration the operation is meant to support.
When the gap is small — typically a few millimeters — the nerve ends can sometimes be mobilized to permit direct repair. When the gap is larger, mobilization is no longer enough, and one of the bridging strategies described below is required.
Nerve Gaps and Why They Matter
A nerve gap exists when the proximal and distal ends cannot be brought together without tension. Gaps occur for several reasons: tissue loss at the time of injury, retraction of the nerve ends after delayed presentation, debridement of damaged segments to reach healthy fascicular tissue, or scar formation that prevents mobilization.
The fundamental challenge of a nerve gap is that the regenerating axons need a pathway. Axons cannot freely cross open tissue and reliably find their target. They need a structural scaffold, ideally with viable Schwann cells, to guide regeneration in the right direction. The longer the gap, the harder this becomes. Short gaps can be bridged by simple conduits. Moderate gaps require allograft material. Long, critical gaps are still best managed with the patient's own nerve tissue.
Gap length is not the only factor. The anatomic location of the injury, whether the nerve is sensory or motor, the distance to the target, the patient's age, and the time elapsed since injury all influence the choice of technique and the likely outcome.
Bridging a Nerve Gap
Three categories of materials are used to bridge nerve gaps. Each has a defined role.
Hollow Conduits
Hollow biological or synthetic conduits — small tubes that span the gap and contain the regenerating axons within a defined channel — work well for short gaps in non-critical sensory nerves. The literature generally supports conduits for gaps of approximately 5 to 10 millimeters in pure sensory nerves. The conduit provides structural guidance but no biological augmentation; the regenerating axons must do all the work themselves. For longer gaps or for motor nerves, conduits alone are not sufficient.
Processed Nerve Allograft
Processed nerve allograft — acellular human (cadaveric) nerve tissue that has been decellularized and processed to retain its extracellular matrix — fills an important middle ground. It provides the structural architecture of nerve tissue, including the basal lamina that guides axonal regeneration, without the live cellular components that would provoke immune rejection. The published literature supports its use for moderate gaps in sensory and mixed nerves, with results that approach autologous graft in many series and avoid the morbidity of harvesting the patient's own nerve. Allograft has become a mainstay of sensory nerve reconstruction in modern practice.
Autologous Nerve Graft
Autologous nerve graft — using the patient's own nerve tissue to bridge the gap — remains the standard for long gaps and for critical motor reconstructions. The most common donor is the sural nerve in the lower leg, which is sensory, expendable, and provides a substantial length of usable graft material. Other donor options include the medial antebrachial cutaneous nerve and the posterior interosseous nerve at the wrist.
The advantage of autologous graft is biological. The graft contains live Schwann cells that actively support regeneration, secreting growth factors and remyelinating regenerating axons in a way no off-the-shelf product fully replicates. The disadvantage is donor site morbidity: harvesting the sural nerve produces a small permanent area of numbness on the lateral foot and ankle, which most patients tolerate well but which is not nothing. In other words, "to pay Peter, you must rob Paul" - you must pay with numbness transferred to the donor site. For long gaps in motor nerves, the biological advantages of autologous graft generally outweigh the donor site cost.
A Brief Note on Nerve Transfers
Nerve transfers — rerouting an expendable nerve branch to power an injured nerve closer to its target — are a powerful tool for proximal injuries, delayed presentations, and situations where the distance to the target makes traditional repair unlikely to succeed in time. A "babysitter" procedure is a related concept: a nerve transfer is performed to maintain the target muscle's neuromuscular junctions while a slower primary repair regenerates, preventing irreversible motor endplate degradation in the meantime.
This is a substantial topic with its own indications, techniques, and outcomes literature. For the detailed discussion, see the [peripheral nerve surgery page].
Outcomes: What Patients Actually Recover
Honest outcomes discussion is essential - almost never is there full recovery to pre-injury function. Nerve repair does not restore normal function in most cases. It restores some function, sometimes a great deal, sometimes very little, and the variation is determined by factors largely beyond the surgeon's or patient's direct control.
Sensory recovery depends on the level of injury (closer to the spinal cord often means worse outcomes), the time to repair, the technique used, and the patient's age. Children recover sensation better than adults. Distal injuries recover better than proximal injuries. Recovery proceeds in a predictable sequence — protective sensation first, then increasingly fine discrimination — and continues for a year or more after the surgical repair. Patients should expect that sensation in the area supplied by the repaired nerve will not be normal, but in many cases will be functional.
Motor recovery is harder to achieve and depends critically on time. Muscles reinnervated within the 12- to 18-month window can recover meaningful strength. Muscles denervated longer than that often remain permanently weak or paralyzed regardless of how technically clean the eventual nerve repair is, because the motor endplates have degraded irreversibly. This is why proximal nerve injuries — where the distance from injury to muscle is long — often require nerve transfer rather than primary repair, even when a direct repair is technically possible.
Permanent dysfunction is a real outcome. Some nerve injuries do not recover meaningful function despite optimal surgical care. The reasons range from delay beyond the biological window, to severe injury that destroyed too much of the nerve substance to host factors (age, comorbidities) that limit regenerative capacity. When primary or graft-based repair is unlikely to restore useful function, options include nerve transfers, tendon transfers (using a working muscle to perform the function of a paralyzed one), or, in some cases, accepting the deficit and focusing on adaptive function.
Neuroma Formation: A Recognized Outcome
A neuroma is a disorganized mass of regenerating axons that forms when nerve regrowth encounters a barrier - basically, it's what happens when a nerve "scars" in place. Two patterns are clinically important.
A secondary neuroma forms at the site of a previously repaired nerve when the repair has failed to allow successful axon passage to the distal segment. Pain, tenderness over the repair site, and a positive Tinel's sign at the neuroma are common findings. Treatment may involve neuroma resection with re-repair, grafting, or a neuroma management procedure such as Regenerative Peripheral Nerve Interface (RPNI), which I discussed in a co-authored multicenter series in Plastic and Reconstructive Surgery — Global Open on RPNI for symptomatic hand and digital neuromas.
A neuroma in continuity forms within an injured nerve that remains anatomically intact but has internal disruption. The nerve looks externally normal or thickened but contains scar tissue and disorganized fascicles internally. These are diagnostically harder than complete transections because the question of whether to operate — and what to do during the operation — depends on whether the nerve is conducting any signal at all, often determined intraoperatively with nerve stimulation.
Recovery and Hand Therapy
Outcomes after nerve repair depend on rehabilitation as much as on surgery. Hand therapy maintains range of motion in the joints supplied by the injured nerve, prevents stiffness, retrains sensory and motor function as it returns, and teaches the patient to interpret early reinnervation signals correctly. Patients who skip therapy generally do not achieve their potential recovery, regardless of how technically clean the surgical repair was. This is true across nerve surgery and is consistent with what my published research on hand therapy timing after flexor tendon repair found in a related context.
Written by Brian P. Kelley, MD — Dual Board-Certified Plastic & Hand SurgeonMedically reviewed: May 4, 2026 · Last updated: May 4, 2026 Educational content. Not a substitute for individualized medical evaluation.
Medical References
- Hooper RC, Cederna PS, Brown DL, Haase SC, Waljee JF, Egeland BM, Kelley BP, Kung TA. Regenerative Peripheral Nerve Interfaces for the Management of Symptomatic Hand and Digital Neuromas. Plastic and Reconstructive Surgery — Global Open. 2020;8(6):e2792. PMID: 32766027.
- Johnson SP, Kelley BP, Waljee JF, Chung KC. Effect of Time to Hand Therapy following Zone II Flexor Tendon Repair. Plastic and Reconstructive Surgery — Global Open. 2020;8(12):e3278. PMID: 33425592.
- Fujihara Y, Kelley BP, Chung KC, Waljee JF. Tendon Transfers for Low and High Ulnar Nerve Palsy. In: Chung KC (ed): Operative Techniques in Hand and Wrist Surgery, 3rd edition. Elsevier.
- American Society for Peripheral Nerve: https://www.peripheralnerve.org/.
- American Society for Surgery of the Hand: https://www.assh.org/.
Related Topics
- Peripheral nerve surgery, RPNI, and TMR
- Acute hand and wrist injuries
- Hand and wrist surgery overview
- Replantation and Revascularization
- Nerve and Tendon Transfers
Closing Disclaimer
This article is educational and does not establish a doctor-patient relationship. It does not replace individualized consultation, examination, or review of personal medical history. Patients with peripheral nerve injuries are encouraged to schedule a consultation to discuss their specific situation and reconstructive options.
Written by Brian P. Kelley, MD — Dual Board-Certified Plastic & Hand Surgeon
Medically reviewed: May 4, 2026 · Last updated: May 4, 2026
Educational content. Not a substitute for individualized medical evaluation.
Patient Testimonials
What are patient's saying about Dr Kelley?
Excelente cirujano! Muchas gracias! Bendiciones al equipo.
Maria Acevedo Espinoza
Want to learn more?
Book a consultation
